Quality account
Quality account for 2024 - 2025
Introduction
Who We Are
Our Services
Our Values
Our Trust in Numbers
Section One
Statement of Quality from the Chief Executive
What is the Quality Account?
Statement of Directors’ Responsibilities in Respect of the Quality Account
Section Two
Our organisation’s strategies in relation to Quality
Update on Our People Plan
Update on our Care Services Strategy
Update on our Quality Strategic Plan – 2025 and beyond
Delivering Our Quality Improvement Priorities 2024/2025
The Quality Dashboard
Patient Safety Incident Response Framework (PSIRF)
Health Inequalities
Our Quality Improvement Priorities for the Forthcoming Year
Development of our Quality Improvement Priorities (QIPs) for 2025/2026
Statements of Assurance from The Board
Review of Services
Clinical Audit
Quality Account 2024/25 – Clinical Audit Projects
Clinical Research
Commissioning for Quality and Innovation (CQUIN)
National Quality Requirements
72-hour follow-up and readmissions
Staff Survey
Community Mental Health Services 2024 Survey results
Care Quality Commission (CQC) Regulation, Ratings, and Improvement Plan
Information Governance
Payment by Results
Learning from Deaths
Patient Safety Incidents
Section Three
Improving the Quality of Our Services
Community Mental Health Transformation
A new approach to patient safety
Adult Eating Disorders Service CONNECT introduces groundbreaking referral criteria adjustment
Our continued commitment to improving NHS care for veterans
How co-production leads to positive practice at Red Kite View
Feel Good Mealtimes
Patient and Carer Experience Team
Celebrating Co-Production and Partnership Work: Inspiring Stories and Developments from the Trust
Positive and Safe Working Group – Working together to reduce the use of restrictive practice
Mental Health Legislation
Sexual Safety
Recognising Success
Positive Practice in Mental Health Awards
Our Chief Exec makes the top 10 across the NHS
Ellen is recognised for her contribution to Leeds
A celebration of Apprenticeship achievements at LYPFT
Improvement Made with Service User Involvement
Guardian of Safe Working for Medical Staff
Patient Advice and Liaison (PALS), concerns, complaints and compliments
Falls and Pressure Ulcer Management
Section Four
Statements from Others on the Quality Account
Acknowledgements
Glossary
Contact us
Introduction
Who we are
We are Leeds and York Partnership NHS Foundation Trust – we provide Specialist Mental Health and Learning Disability Services to the people of Leeds and York as well as regionally and nationally.
Our vision is to provide outstanding Mental Health and Learning Disability Services as an employer of choice. This means supporting our service users and carers, our staff and the communities we serve, to live healthy and fulfilling lives where we can all achieve our personal and professional goals, and live free from stigma and discrimination.
We offer services to people who need support and treatment for a wide range of mental health conditions, from depression, anxiety, and obsessive-compulsive disorder, to dementia, bipolar disorder, schizophrenia and personality disorders.
We support people living with issues such as addictions, eating disorders, or physical problems with psychological causes, and those needing the support of our Gender Identity Service.
We offer community, supported living and respite care to people with varying degrees of learning disabilities, physical disabilities, and complex needs. We offer services across the region, and in a variety of locations, including Inpatient Children’s Services in Leeds and York, Deaf Children’s Services across northern England, and Secure Services for Leeds and York.
Much of our care is provided in, or close to, people’s own homes with the need for people to stay in hospital kept to a minimum.
We are an NHS Foundation organisation, which means:
- We have some freedoms to decide locally how to meet our requirements.
- We are accountable to the people within our communities, who can become members and governors.
- The Trust is independently regulated and inspected by the Care Quality Commission (CQC).
Our Services
Here’s a summary of our services, you can visit our services for more details about these:
- 18-25 Deaf Mental Health Assessment Service
- Acute Inpatient Service
- Adult Attention Deficit Hyperactivity Disorder (ADHD) Service
- Alcohol and Drug services: Forward Leeds
- Assertive Outreach Team
- Autism Diagnostic Service (LADS)
- Blue Light (emergency services mental health support)
- Care Homes Team
- Child and Adolescent Mental Health Service – York and North Yorkshire
- Children and Young Peoples Mental Health Service (CYPMHS) Inpatient Unit for West Yorkshire
- Community Learning Disability Teams (CLDT)
- Community Mental Health Service
- Community Rehabilitation Enhanced Support Team (CREST)
- Complex (Locked) Rehabilitation – Newsam Centre Ward 5
- Complex Dementia Wraparound Team
- Crisis Assessment Unit
- Crisis Resolution Intensive Support Service
- Deaf Child and Adolescent Mental Health Service (Deaf CAMHS)
- Eating Disorder Service (Adult)
- EMERGE Leeds: Complex Emotional Needs Service
- Gender Identity Service
- Healthy Living Service
- Intensive Home Treatment Team for Older People (IHTT)
- Intensive Care Homes Treatment Team for Older People (ICHTT)
- Learning Disability Inpatient Services
- Learning Disability Specialist Health Planned Care (Respite)
- Leeds Psychosexual Medicine Service (PSM)
- Liaison Psychiatry
- Low Secure Forensic Services – Leeds and York
- ME/CFS Service (Chronic Fatigue Syndrome/Myalgia Encephalomyelitis)
- Memory Assessment Service
- National Inpatient Centre for Psychological Medicine (NICPM)
- Northern Gambling Service
- Older Peoples Inpatient Services
- Older Peoples Community Services
- Op Courage – Veterans Mental Health Services
- Pathway Development Service – Yorkshire and Humberside
- Perinatal Mental Health Service
- Psychiatric Intensive Care Service (PICU)
- Rehabilitation and Recovery Services
- Rough Sleepers Mental Health Service (RSMHS)
- Specialist Supported Living Service (SSLS)
- Younger People with Dementia Service
Our Values
Our values are integrity, simplicity, and caring. They are integral to how we go about our business. The way we behave and interact with one another is central to living our values.
| Our values | Behaviours that uphold our values |
| We have integrity We treat everyone with respect and dignity, honour our commitments and do our best for our service users and colleagues. |
|
| We keep it simple We make it easy for the communities we serve and the people who work here to achieve their goals. |
|
| We are caring We always show empathy and support those in need. |
|
Our Trust in Numbers
- 811,000 plus people we provide services to
- 35 services we provide
- Good our overall CQC rating
- £277.4 million annual turnover for 2024/2025
- 60 sites we operate from
Our services and service users:
- 631 compliments received by the Trust in 2024/2025
- 85% of staff feel their role makes a different to service users
- 189 service users and carers are members of our Service User Network
Our people:
- 3,365 substantive staff
- 590 flexible staff
- 588 medical staff, including consultants, doctors and registrars
- 871 other clinical staff, including healthcare support workers
- 882 registered nursing and midwifery staff
- 286 other professional, scientific and technical staff, including psychologists, psychotherapists and pharmacists
- 229 allied health professionals, including occupational therapists and dieticians
- 887 admin, estates, and non-clinical staff
- 170 members of our Workforce Race Equality Network (WREN)
- 91 members of our Disability and Wellbeing Network (DaWN)
- 102 members of our Rainbow Alliance
Our Trust online
- 111 Facebook posts
- 82 X posts
- 4,239 page fans on Facebook
- 9,187 X followers
- 18,106 LinkedIn followers
- 268 Instagram followers
- 2,320 YouTube Subscribers
- 11,553 the average number of visitors to our website each month
Our research
- 39 research studies the Trust was involved in during 2024/2025
- 275 people took part in research hosted or led by the Trust in 2024/2025
- £1.4 million received in research grants from the National Institute for Health Research and other funders in 2024/2025
Section One
Statement of Quality from the Chief Executive
Dr Sara Munro, Chief Executive 
As we reflect on the past year at Leeds and York Partnership NHS Foundation Trust, I want to express my gratitude to our dedicated staff, service users, and partners. Despite the challenges, we have made significant progress in improving mental health services, tackling inequalities, and fostering a culture of compassion and innovation. I am privileged to lead such committed and talented people who work tirelessly all year round to provide great care or who provide the conditions for great care to happen.
The increasing demand for mental health services, particularly in Adult Acute Care, has required a concerted effort from our teams. Through our Improving Patient Flow programme, we have significantly reduced out-of-area placements, enhanced timely discharges, and improved bed management to ensure that those in crisis receive the right support at the right time. The launch of the NHS 111 mental health helpline has provided a crucial lifeline for those in urgent need. At the same time, a new pilot scheme allows our acute teams to respond to certain mental health-related 999 calls, reducing unnecessary hospital admissions and improving crisis response.
The transformation of Community Mental Health Services across Leeds has gained momentum, with our early implementer sites showing promising results. Our Crisis Resolution Intensive Support Service (CRISS) has been restructured into three crisis and home treatment teams, ensuring a more streamlined and effective service. We have continued strengthening our partnerships with primary care and voluntary sector organisations to provide holistic and accessible mental health support.
Our Adult ADHD Service has faced difficult but necessary decisions, including pausing non-urgent referrals to focus on those with the greatest clinical need. At the same time, we developed a sustainable, long-term solution that improves access for all. The National Deaf Child and Adolescent Mental Health (North) Service is running a mental health assessment service for deaf adults aged 18-25; the pilot programme will provide an assessment/diagnostic service, with short-term intervention sessions where appropriate, at our site in York.
We know that people with serious mental illness die on average 15 to 20 years earlier than the general population. Additionally, individuals with a learning disability are 3 to 4 times more likely to die from avoidable medical causes. Those with neurodiverse conditions often face significant challenges in accessing timely services and treatments, which results in poorer health and reduced life opportunities. Addressing health inequalities remains at the core of our mission. Our first Improving Health Equity Strategy, led by our Chief Operating Officer Joanna Forster Adams, Head of Health Equity Sophie Valinakis and Dr Anna Ray, our Consultant in Public Health, provides a framework to ensure better access to services and improved health outcomes. By embedding health equity principles across our organisation, we are taking meaningful steps to bridge gaps in care and tackle the social determinants of health that disproportionately affect the people we serve.
Supporting our staff remains a top priority. We recognise our teams’ immense dedication and hard work and are committed to fostering a positive and inclusive workplace culture. We continue to prioritise wellbeing initiatives to support staff retention and satisfaction, and our “Spotlight” recognition platform has empowered colleagues to celebrate each other’s contributions. I am committed to supporting the Spotlight platform and taking the opportunity to recognise individuals and teams every week for their work. This year, many of our colleagues have received national awards and accreditations, showing how we are “leading the way in mental health, learning disability and neurodiversity care.”
Our Chaplaincy Team has continued its journey to becoming multi-faith with two new members and have seen the distribution of multi-faith chaplaincy resource boxes and training for staff on supporting service users from different faith backgrounds. They have introduced drop-in events and multi-faith room user group meetings to meet the needs of those who use them. Looking ahead, volunteer chaplains from diverse faith communities will begin offering support across multiple sites, further strengthening our inclusive approach to spiritual care.
We remain committed to fostering an inclusive and supportive workplace. Our values-based recruitment programme has progressed, ensuring we recognise lived experience as an asset. We also continue to embed collective leadership, strengthening collaboration across teams.
Our partnerships with local organisations and research institutions have driven innovation in mental health services. This year, we launched a new clinical research hub, furthering our commitment to evidence-based practice. We have also continued our collaboration with third-sector partners, delivering impactful initiatives to support mental health recovery and wellbeing in the community.
Financial sustainability has also been a focus, and through careful planning, we have reduced our reliance on agency staff and identified efficiencies in corporate services to ensure that we direct our resources towards frontline care. Additionally, significant investment has gone into upgrading our digital infrastructure to improve accessibility and efficiency. Introducing an electronic document management system has streamlined administrative processes, enabling clinicians to spend more time with patients.
Patient safety remains at the heart of everything we do. In 2024, we adopted the Patient Safety Incident Response Framework (PSIRF), shifting towards a learning-focused, non-punitive approach to incident management. This new model reinforces our commitment to transparency, fairness, and continuous learning, ensuring that we apply insights from past experiences to improve outcomes for our service users.
The redevelopment of Parkside Lodge as the new home for our High-Intensity Rehabilitation Service marks a major milestone, ensuring that those with complex needs receive high-quality, person-centred care in a modern and supportive environment and adapting to new national commissioning guidelines. These infrastructure improvements are a testament to our commitment to innovation and service enhancement.
Our Perinatal Mental Health Service received a boost from the Care Quality Commission (CQC) following an unannounced inspection earlier in the year. The CQC gave them an overall rating of ‘good’. The inspection team said we should be “pleased with the findings of [their] report, which highlights many areas of good practice and a positive environment for people needing help and support.” In April 2025, we will take on the role of lead provider for perinatal mental health services within the region, with plans to expand inpatient care for mothers and babies later in the year.
Our refreshed five-year strategy, Improving the Health and Lives of the Communities We Serve, will shape our priorities and drive forward innovation, integration, and person-centred care, describing who we are, where we are going and how we plan to get there. The strategy also showed off our refreshed brand and visual identity, which we had spent the previous year co-developing with staff, people with lived experience, and health and care partners. One specific element of our refreshed brand is our new Trust strapline, developed in response to feedback about the ambiguity of the Trust’s name. The strapline we adopted is:
“Leading the way in mental health, learning disability and neurodiversity care.”
I want to sincerely thank our staff, service users, and partners for their unwavering dedication, resilience, and passion. Your commitment makes a real difference in people’s lives.
What is the Quality Account?
Once a year, every NHS Trust is required to produce and publish a Quality Account. The account is a look back over the year to show how we have improved the quality of our services, a look forward at what our plans are for the coming year and an explanation of who we are.
This Quality Account is for service users, carers, and members of the public. The aim is to make sure that everyone who would like to know about our services can access this information.
What’s included?
The core elements of a Quality Account are:
- How we performed last year (2024-25), both through our prioritised activities and through other quality improvement work.
- The information we are required by law to provide – this is reported in a very strict way so that we can be compared to other NHS Organisations.
- What we plan to do next year (2025-26), why we have chosen these priorities, and how we will go about it.
Statement of Directors’ Responsibilities in Respect of the Quality Account
Organisations are required under the Health Act 2009 and subsequent Health and Social Care Act 2012 to produce Quality Accounts. NHS England has issued guidance on the required indicators within Quality Account. In preparing the Quality Account, Directors are required to take steps to satisfy themselves that:
- The content of the Quality Account is not inconsistent with internal and external sources of information including:
- Board minutes and papers for the period April 2024 to March 2025
- Papers relating to quality reported to the Board over the period April 2024 to March 2025
- Feedback from local Healthwatch organisation dated June 2025
- The Quality Account presents a balanced picture of the NHS Foundation Organisation’s performance over the period covered.
- The performance information reported in the Quality Account is reliable and accurate.
- The Quality Account has been prepared in accordance with NHS England’s guidance.
- The Directors confirm to the best of their knowledge and belief they have complied with the above requirements in preparing the Quality Account.
By order of the Board.
Date: June 2025
Chair: Merran McRae
Section Two
Our organisation’s strategies in relation to Quality
Improving the Health and Lives of the Communities we Serve: from 2025 to 2030 is the new five-year strategy of Leeds and York Partnership NHS Foundation Trust.
Read our strategy, and its underpinning five strategic plans.
Our Strapline
Leading the way in mental health, learning disability and neurodiversity care.
Our Vision (where we want to be)
To lead the way in mental health, learning disability and neurodiversity care so the communities we serve can live healthy and fulfilling lives, our people can achieve their personal and professional goals, and everyone can live their lives free from stigma and discrimination.
Our Mission (how we want to get there)
To improve the health and lives of the communities we serve by providing outstanding mental health, learning disability and neurodiversity services; to be a great place to work and a great partner to work with.
Update on Our People Plan
Darren Skinner – Director of People and Organisational Development
Great care is delivered by great people, and we know that to continue to provide high-quality healthcare services, we need to support our colleagues to be the best they can be at work. In recent years, those working in the NHS have continued to rise to considerable challenges, and our People Plan has been developed, and continues to evolve, with this in mind.
It is our commitment to all our colleagues to help improve their working experience, so they are prepared and supported for whatever lies ahead. The People Plan indicates what those who work at Leeds and York Partnership NHS Foundation Trust (LYPFT) can expect from us and each other and sets out what we want to achieve under each of the four NHS People Plan ambitions – looking after our people, belonging in the NHS, new ways of working and delivering care, and growing for the future.
Our vision will be delivered through four strategic ambitions for our people. In developing this plan, our organisation has considered both local and national people priorities, including the NHS Long Term Workforce Plan 2023, the NHS People Plan 2020/21 and the seven NHS People Promises. The People Plan sets out what the people of the NHS can expect – from their leaders and from each other. It focuses on:
- Looking after our people, particularly the actions we must all take to keep our people safe, healthy, and well – both physically and psychologically.
- Belonging in the NHS, highlighting the support and action needed to create an organisational culture where everyone feels they belong.
- New ways of working and delivering care, emphasising that we need to make effective use of the full range of our people’s skills and experience to deliver the best possible patient care.
- Growing for the future, particularly by building on the renewed interest in NHS careers to expand and develop our workforce, as well as retaining colleagues for longer.
Our People Plan 2024-27 reflects the strategic direction in the NHS People Plan and the NHS People Promise, and the four strategic ambitions reflect the national priorities. It builds upon the success of our previous 2021-2024 People Plan. Visit the our strategy page to read the People Plan.
Road map: making sure we deliver
The People Plan will be delivered through a Road Map which will set out key actions and milestones for 2024-2027. We will use the Road Map to plan our work, report progress and hold ourselves to account. Outcome We have developed a set of success measures which are set out in our performance dashboard. These success measures are unique to each iteration of our People Plan and have helped shape the objectives for 2024-2027, based on the successes of the previous plan. Reporting and review Progress on the delivery of the Road Map and success measures will be reviewed regularly and reported to the following groups, at a frequency agreed through the People and Organisational Development Governance Groups.
Update on our Care Services Strategy
Joanna Forster Adams – Chief Operating Officer 
We have a clear ambition for what we want to deliver in the future, who will deliver care services, where care services will be delivered and how care services will be delivered in the future. These all link to our overarching organisation’s vision to provide outstanding mental health and learning disability services as an employer of choice.
People are at the heart of everything we do both those who we partner with to deliver care, and our teams. We will harness opportunities to understand our other health and care partners and population and work more collaboratively together. By doing this, we will deliver high quality care to all our people. Our ambitions align with our objectives to tackle health inequalities with a specific focus on access, experience and physical health.
To bring our ambition to life, we have refreshed our priorities and focus for the next 5-10 years and have set ourselves objectives to deliver on:
- We co-create and co-deliver care services with people who have lived experience
- We collaborate with our partners to understand our populations and provide proactive integrated care
- We provide high quality, equitable and sustainable care services
For further information regarding this strategy, please access the 2023-2028 Care Services Strategic Plan on our strategy page.
Update on our Quality Strategic Plan – 2025 and beyond
Dr Chris Hosker, Medical Director 
At our Trust, we’re dedicated to providing the best possible care. Our Quality Strategic Plan for 2025 and beyond focuses on creating the right environment for high-quality care throughout our organisation.
What Quality Means to Us
Quality can have different meanings for different people. For us, it means making sure your healthcare is:
- Safe: Protecting you from harm.
- Timely: Reducing waits and delays.
- Effective: Providing care that works.
- Efficient: Making the best use of resources.
- Equitable: Ensuring fair access for everyone.
- Person-centred: Putting you at the heart of everything we do.
These six principles – Safe, Timely, Effective, Efficient, Equitable, and Person-centred (STEEEP) – guide all our actions.

The STEEEP framework for healthcare quality is illustrated in a circular diagram with six segments: Safe (pink, umbrella icon), Timely (purple, clock icon), Person Centred (green, two people icon), Equitable (orange, balanced scales icon), Efficient (blue, gear icons), and Effective (teal, atom icon). At the center is the acronym “STEEEP” in blue capital letters.
Building on Our Past
We launched our first Quality Strategic Plan in 2018 after speaking with our Council of Governors, Board members, senior leaders, and staff. This plan helped us improve care until January 2024, when we updated it to meet new challenges and opportunities. The updated plan for 2024 and beyond was agreed by the Board, and it’s built on the idea that our organisation exists to provide high-quality, continuously improving care, every time you interact with our services.
Our Beliefs About Quality Care
We believe quality care begins with the connection between you and our clinicians. To make this happen, we need to:
- Recognise that our work is often complex.
- Bring together the knowledge of many people to achieve the best results.
- Create the right conditions for quality care to flourish.
- Use our Quality Strategic Plan as a roadmap to deliver better care and support our staff.
- Provide a framework to deliver the right care, every time.
- Acknowledge the challenges that come with improving quality.
- Empower our staff to take ownership of quality while ensuring consistency across the organisation.
- Combine the best international evidence with the experiences of our service users, carers, and staff.
Our Vision and Priorities
Our vision is to provide outstanding Mental Health and Learning Disability Services, whilst being an employer of choice. We want to support you, our staff, and the wider community to live healthy and fulfilling lives. To achieve this, we focus on:
- STEEEP Care: Making sure our care is safe, timely, effective, efficient, equitable, and person-centred.
- Empowering Staff: Encouraging everyone to take ownership of quality.
- Learning and Improving: Using the best evidence and listening to your experiences to drive change.
- Putting You First: Keeping you, your carers, and families at the heart of our work.
How We Improve Quality
Our approach focuses on five key areas:
- Pro-Quality Conditions: Using evidence to build an environment where quality care can thrive.
- Knowing How We are Doing: Tracking progress and communicating effectively from frontline staff to the Board.
- Help and Support: Offering joined-up support where it is needed most.
- Priorities: Developing systems to set and deliver priorities fairly.
- Work Across Boundaries: Collaborating across different teams and systems to deliver high-quality care.

An infographic showing a circular model for achieving quality care in healthcare. It emphasises the importance of performance monitoring, creating conditions that support quality, working collaboratively across boundaries, setting clear priorities, and offering appropriate help and support.
Measuring and Improving Quality
We use several ways to measure quality, such as service visits and peer reviews, feedback from the Care Quality Commission (CQC), compliments, complaints, and your feedback and outcome measures and performance reports.
In the future, we will also:
- Use data and peer visits to identify where teams need support.
- Create better electronic systems to help teams track improvements.
- Strengthen peer support and learning across the organisation.
Setting Priorities Together 
Priorities can change as we learn and grow. That is why we will work with service users, staff and carers to set and revise priorities, to make sure they reflect their needs. We want to encourage teams to implement their ideas and will offer support for bigger changes that affect multiple services and the system.
The flower-shaped infographic illustrates the components of shared values and leadership in healthcare. The petals highlight Shared Workforce, Coordination of Care, Shared Leadership, Information Sharing, and Prevention and Self Care, all centred around Shared Assessment. The roots and stem symbolise the foundational elements of Leadership, Culture, and Learning, supported by Stakeholders and Partnerships.
Looking Ahead
Over the next year, we will focus on:
- Amplifying staff, service user and carer voices and experiences to bring our plan to life.
- Strengthening collective leadership and collaboration.
- Providing targeted support where it’s needed most.
By staying true to our values and working together, we’re confident that our Quality Strategic Plan for 2025 and beyond will help us deliver the high-quality care you deserve.
Delivering Our Quality Improvement Priorities 2024/2025
Our 2024/25 Quality Improvement Priorities (QIPs)
Following a discussion at Executive Management Team in April 2023 and agreement at Board in June 2023, three Strategic Quality Improvement Priorities for 2024/25 were identified for our organisation:
- The Quality Dashboard is a way of displaying various types of visual data in one place to help monitor and improve the quality of care.
- The implementation of Patient Safety Incident Response Framework sets out the way that our organisation will respond to patient safety incidents.
- Health Inequalities is about the differences in the care that people receive and the opportunities that they have to lead healthy lives.
The Quality Dashboard
‘Knowing how we are doing’ is a key component of our organisation’s Quality Strategic Plan. Knowing the quality, strengths and weaknesses of our teams and services – the ‘bright lights and hot spots’ will identify the good practice we can learn from and where more support is needed, which will help us become more effective.
Vision
Across our organisation, we already have many ways of assessing quality. These include service visits and peer reviews; the metrics that make up our combined quality and performance report to our Board, Care Quality Commission feedback, compliments, complaints and service user feedback and outcome measures. The vision is to have the right integrated data at every level – from supporting individuals’ care, understanding services and how they are functioning, to leading and managing our organisation.
Aim
To develop a systematic integrated dashboard system that will meet the needs of the entire organisation from all perspectives.
Our progress
Developing Measures for the Quality Database
As part of our ongoing work to strengthen our approach to understanding and improving quality, we have been developing a core set of measures to be included within our Quality Database. This work is focused on ensuring that the data we collect is both meaningful and useful in helping us understand how services are performing and where improvements can be made.
Our approach so far has included:
- Reviewing what we currently measure and why – taking stock of the data we already collect across services, and the original purpose behind these measures.
- Interpreting what the data tells us – recognising that the same metric can carry different meanings depending on the context of the service, its size, population, or model of care.
- Identifying useful measures for different audiences – ensuring the selected measures can support learning and decision-making at both the team level and at Board level.
- Creating an initial list of proposed measures – based on the above, we have drafted a starting set of indicators that we believe could offer valuable insights into service quality.
We are now moving into a testing phase, where we will begin using these measures in practice. This work relates to the Quality Strategic Plan, and specifically the knowing how we are doing element.
The feedback from this phase will help shape the final set of measures used within the Quality Database and ensure that our approach remains grounded, relevant, and responsive to the needs of services and the people they support.
Patient Safety Incident Response Framework (PSIRF)
The Patient Safety Incident Response Framework (PSIRF) is a new national mandatory framework to help ensure people are protected from avoidable harm and abuse and improve our learning when things do not go as planned.
PSIRF sets out the way that our organisation will respond to patient safety incidents. It focuses on system-based learning and involves working in collaboration with service users, families and carers and explores a wider range of patient safety incidents, in the spirit of using reflection, openness, fairness and learning. The framework sets out the NHS’s approach to developing and maintaining effective systems and processes for responding to patient safety incidents for the purpose of learning and improving patient safety.
PSIRF allows us to focus on areas with the greatest potential for patient safety improvement, ultimately making care safer for our patients. PSIRF supports the key principles of a patient safety and just culture, focusing on understanding how incidents happen, rather than apportioning blame, allowing for more effective learning.
Vision
The vision for our organisation is a cultural shift in the way we respond to patient safety incidents and supports the development and maintenance of an effective patient safety incident response system.
Aim
To fully embed the PSIRF approach and systems across all aspects of responding to, investigating, and learning from incidents that occur across our organisation.
Our progress
Policy and plan
Our organisation has developed and implemented a Patient Safety Incident Response Framework policy in July 2024. This policy supports the requirements of the NHS England Patient Safety Incident Response Framework (PSIRF) and sets out how we will approach the development and maintenance of effective systems and processes for responding to patient safety incidents and issues, for the purpose of learning and improving patient safety. The policy supports development and maintenance of an effective systems that integrate the four key aims of the PSIRF, which we can also align to our existing Trust values:
- Compassionate engagement and involvement of those affected by patient safety incidents (Integrity, Caring)
- Application of a range of system-based approaches to learning from patient safety incidents (Integrity)
- Considered and proportionate responses to patient safety incidents and safety issues (Integrity, simplicity)
- Supportive oversight focused on strengthening response system functioning and improvement. (Integrity, simplicity, caring)
Our patient safety incident response plan sets out how we intend to respond to patient safety incidents from May 2024-November 2025. The plan will remain flexible and consider the specific circumstances in which patient safety issues and incidents occurred and the needs of those affected.
The plan is a ‘living document’ that will be appropriately amended and updated as we use it to respond to patient safety incidents. We will review the plan as a minimum every 18 months to ensure our focus remains up to date, with ongoing improvement work. We recognise that our patient safety incident profile may also require change. This will also provide an opportunity to re-engage with stakeholders to discuss and agree any changes made in the previous term. Updated plans will be published on our website, replacing the previous version. A rigorous planning exercise will be undertaken every four years and more frequently if appropriate, as agreed with our integrated care board (ICB) to ensure efforts continue to be balanced between learning and improvement.
Learning responses and training
Our organisation initiated a robust training programme around patient safety and the learning response frameworks that are now used, in conjunction with the launch of PSIRF in June 2024.
Level one – Essential of Patient Safety
This is mandatory training for all staff, clinical and non-clinical. To date, 3138 staff members have completed this training. This equals to 84% of the substantive and fixed term workforce.
Patient Safety Level 2 – Access to Practice
All clinical staff at AFC Band 6 or above, or those with potential to support or lead patient safety incident management are required to complete this training.
After Action Review
An After-Action Review (AAR) is a method of evaluation that is used following incidents. It aims to capture early learning to avoid failure and promote learning for the future.
Our organisation aims to have 300 active members of staff that are trained to facilitate AAR at any given time. To date 210 staff members have completed this training.
Patient Safety Incidents Investigations
A patient safety incident investigation (PSII) is undertaken when an incident or near-miss indicates significant patient safety risks and potential for new learning. Our organisation has clinical staff as well as staff within the Nursing and Professions, Quality and Patient Safety departments, who have completed external training in carrying out Patient Safety Incidents Investigations.
Thematic Review
A Thematic Review can identify patterns in data to help answer questions, show links or identify issues. Thematic Reviews are currently being supported directly by Patient Safety Managers. In-house training has been developed on both these PSIRF review methodologies and trainings, and the first two cohorts have been launched.
Patient Safety Partners
The Patient Safety Partner (PSP) is a new and evolving role developed by NHS England / Improvement as part of the NHS Patient Safety Strategy (July 2019) to help improve patient safety across the NHS in the UK. Within our organisation, we are welcoming PSPs to offer support alongside our staff, patients, families/carers to influence and improve safety across our range of services. PSPs can be patients, carers, family members or other lay and this offers a great opportunity to share interests, experiences, and skills to help develop the new PSP role and be a part of our team.
The organisation will be looking to embed these roles within the next financial year.
Health Inequalities
Ensuring that the care we provide to our service users is equitable and responsive to the diverse needs of our health populations with compassion, dignity, and respect.
Health inequalities are the systematic, unfair, and avoidable differences in health across the population, and between different groups in society. Health inequalities are ultimately about differences in the status of people’s health. Inequalities result from the conditions in which we are born, grow, live and work, and from our access and experience of health care.
We are concerned with inequity between multiple groups in society which include those living in deprived communities, people with protected characteristics, inequalities in geography (such as rural versus urban) and inclusion health groups (such as those experiencing homelessness or sex workers).
Our organisation recognises that everyone deserves high quality healthcare, and we are committed to continue our work to actively reduce health inequalities. As a provider of specialist mental health and learning disability services, we know that people living with mental illness and learning disability are at a higher risk of developing physical health problems.
Vision
Access – ensuring that access to our services is available to all, with nobody accidentally excluded, with access that suits the needs of individuals and communities across our footprint (including relatable, culturally competent in-reach and appropriate adaptations).
Experience – ensuring that people’s experience of our services, care, treatment, and support is not affected by any characteristic.
Improve, and advocate for, the physical health of people with mental ill health and/or learning disabilities.
Aim
To develop and publish a new Health Inequalities Strategy and Action Plan.
To purposefully address the inequity, we know already exists in Mental Health and Learning Disability services and in their delivery.
Our progress
Strategy
Our Improving Health Equity Strategic Plan, 2025-2029 has been developed through engagement with a broad range of LYPFT colleagues and system partners. We engaged with over 500 people, meeting individually with key stakeholders and through various forums such as the Service User Network, staff networks, trust wide governance meetings and system partnership meetings. We hosted an open access webinar where attendees from across the Trust and West Yorkshire Partners had the opportunity to influence the development of our Strategic Plan.
This plan will largely focus on improving equity in access, experience and outcomes within healthcare. We are particularly concentrating on the following groups:
- The systematic, unfair and avoidable differences in health between those with learning disability, neurodiversity*, severe and enduring mental illness, and those without.
- Tackling racial health inequity within mental health services which have been evidenced to be extensive and persistent.
- Intersectionality: People at exceptionally high risk of poor health outcomes because they are a member of multiple groups and experience compounding disadvantage for example those with a severe mental illness and from a racialised community and who also live in a deprived community.
- Our service users who experience deprivation, with a particular focus on our service users living in the 10% most deprived communities nationally.
Visit the Improving Health Equity page to learn more.
Patient Carer Race Equality Framework (PCREF)
PCREF is the first ever anti-racism framework from NHSE, and our organisation been selected to be one of the national early implementer sites. This work brings ground-breaking change to our sector, building on progress we have achieved locally, and promoting a whole new dimension of coproduction, where individuals and communities are at the heart of the design and implementation of the services they need.
This agenda will enable us to focus our efforts and progress our journey to becoming an actively anti-racist organisation by ensuring that we are responsible for co-producing and implementing concrete actions to improve racial equity within our services. It will also become part of Care Quality Commission (CQC) inspections.
It supports improvement through three domains including:
- Leadership and governance: Trusts’ boards will be leading on establishing and monitoring concrete plans of action to reduce health inequalities.
- Feedback mechanisms: visible and effective ways for patients and carers to feedback will be established, as well as clear processes to act and report on that feedback.
- Organisational competencies: measurable and practical actions to ensure that the whole organisation is aware of its responsibilities.
As an NHS Mental Health provider of services, we are mandated to deliver against the PCREF and publish our plan of action.
Workforce development
In 2024, 182 staff received Cultural competency and Humility Training. This course is delivered to healthcare professionals to become aware of their own cultural norms, examine their own ideas about personal biases, stereotypes and prejudices. The training explores why inequalities exist and persist and empower services to become more culturally responsive to help improve equity and health outcomes in our populations.
Our organisation is entering the third year of our support in delivering the ‘Improving Population Health Fellowship Programme’. Four members of staff have been successful in applying in becoming Health Equity Fellows for 2025/26. Our new cohort of fellows will carry out projects to support improving health equity and help make Leeds and York Partnership NHS Foundation Trust, and the wider West Yorkshire system equity informed.
Synergi Leeds Partnership
![]() Our organisation has funded the creation of an ambitious digital archive that highlights the untold contributions of communities and grass root organisations who have worked tirelessly across the city to address ethnic inequalities in mental health. The project has been a collaboration between ‘Words of Colour’, the Trust, Public Health, Forum Central and other stakeholders across the city, including Leeds Playhouse, Thackeray Museum and other creative individuals and organisations.
Our organisation has funded the creation of an ambitious digital archive that highlights the untold contributions of communities and grass root organisations who have worked tirelessly across the city to address ethnic inequalities in mental health. The project has been a collaboration between ‘Words of Colour’, the Trust, Public Health, Forum Central and other stakeholders across the city, including Leeds Playhouse, Thackeray Museum and other creative individuals and organisations.
Learn more about Synergi Leeds.
Our Quality Improvement Priorities for the Forthcoming Year
Development of our Quality Improvement Priorities (QIPs) for 2025/2026
It was proposed in December that the current Quality Improvement Priorities (QIPs) are continued for another year. The Trusts current QIPS are:
- Implementation of the Patient Safety Incident Response Framework (PSIRF)
- Health Inequalities
- Quality Dashboard
The rationale for this was to continue the work that is currently underway and ensure that improvements are fully embedded within the organisation, enabling us to demonstrate the impact. The proposal was taken to the Quality Committee, and a request was made for this to go to the Trust Board in January for a final decision. It was subsequently agreed at the Trust Board that the 2023/2024 QIPs will continue into 2025/2026.
To ensure ongoing oversight of the QIPS, each lead will be asked to describe how they will monitor and evaluate the embedding and impact of the priorities over the next 12 months. An update will then be provided via the related governance route, with a report to Quality Committee.
Discussions are ongoing on future QIPs and how these can be aligned to the Trusts Quality Strategic Plan.
Statements of Assurance from The Board
This section has a pre-determined content and statements that provide assurance about the quality of our services in our organisation. This information is provided in common across all Quality Accounts nationally, allowing for comparison of our services with other organisations. The statements evidence that we are measuring our clinical services, process, and performance and that we are involved in work and initiatives that aims to improve quality.
Review of Services
During 2024/25 our organisation provided and/or sub-contracted around 30 NHS services. Our organisation has reviewed all the data available to us on the quality of care in all these services. Our organisation has taken the following actions to further improve data quality during the year:
- We have continued to embed operational dashboards focused on improving awareness to missing, poor quality or incorrect data recording within Care Director and our Business Intelligence tool and have worked to embed this into clinical practice via the Digital Change Leads and Data teams.
- We have further improved the documentation and visibility of processes used to monitor and publish performance against national and contractual data quality metrics to provide broader organisational understanding.
- We have supported external audits of data quality.
- We have run local quarterly data quality audits to understand where data quality is impacting on key performance measures. The results were shared with the relevant services and support given to understand what changes are required where appropriate.
- Despite our clinical system supplier exiting the mental health market, we continue to review core processes within Care Director to ensure that data quality issues are resolved as close to the point of data entry as possible and explore automated updating and creation of records following events such as admissions to our inpatient services and discharges.
- We have continued to raise awareness throughout the organisation of key clinical record keeping processes that impact on data quality and performance including an update to the Data Quality Policy.
- We have continued to embed the importance of data quality to assist teams in identifying and resolving data quality issues.
- We have continued to monitor and raise awareness of performance against national and contractual data quality metrics.
LYPFT will be taking the following actions to improve data quality during 2024/25:
- Enhanced monitoring of data completeness and quality.
- Continue to support to staff in utilising Care Director effectively.
- Continue to deliver a programme of data quality audits.
- Continue to raise awareness throughout the organisation of key clinical record keeping processes that impact on data quality and performance.
- Continue work with the Improvement Team to design and implement a Quality Dashboard. We hope this will build upon the STEEEP (Safe, Timely, Effective, Efficient, Equitable and Patient-centred) framework and connect quality metrics at the frontline to those reviewed at the Board. More information about this can be found in the Quality Improvement section of this document.
The income generated by the relevant health services reviewed in 2023/24 represents 100% of the total income generated from the provision of relevant health services by our organisation for 2023/24.
Mental Health Services Data Set – Data Quality Maturity Index
Leeds and York Partnership NHS Foundation Trust submitted data during 2024/25 to NHS Digital / NHS England via the Mental Health Services Data Set which are included in the latest Data Quality Maturity Index published data (December 2024 published March 2025). The percentage of records in the published data:
-
- That included the patients valid NHS Number was 99%.
- That included the patient’s valid General Medical Practice Code was 100%.
- That included the person stated gender code and gender identity code combined was 98%.
Clinical Audit
Quality Account 2024/25 – Clinical Audit Projects
“Clinical audit is a way to find out if healthcare is being provided in line with standards and let’s care providers and patients know where their service is doing well, and where there could be improvements.
The aim is to allow quality improvement to take place where it will be most helpful and will improve outcomes for patients.” NHS England (2023)
National Clinical Audits
During 2024/25 six national clinical audits and two national confidential inquiries covered the NHS services that Leeds and York Partnership NHS Foundation Trust provides.
The below table shows list of national clinical audits and national confidential enquiries that Leeds and York Partnership NHS Foundation Trust was eligible to participate in during 2024/25:
Table one – LYPFT Eligible national clinical audits and national confidential enquiries
| Eligible National Clinical Audits participated in |
| National audit of Inpatient Falls (NAIF) |
| POMH-UK topic 21b: The use of melatonin |
| POMH-UK topic 24a: Opioid medications in mental health service POMH-UK topic 18c: Use of Clozapine National Audit of Care at the End of Life (NACEL) Mental Health Spotlight Audit 2025 National Audit of Eating Disorders (NAED) 2024/27 |
| Eligible National Confidential Enquiries participated in |
| Mental Health Clinical Outcome Review Programme – National Confidential Inquiry into Suicide and Homicide by People with Mental Illness |
| Learning Disabilities Mortality Review (LeDeR) |
The national clinical audits and national confidential enquiries that Leeds and York Partnership NHS Foundation Trust participated in, and for which data collection was completed during 2024/25 are listed below alongside the number of cases submitted to each audit or enquiry as a percentage of the number of registered cases required by the terms of that audit or enquiry.
Table two – National clinical audits and national confidential enquiries that LYPFT participated in, and for which data collection was completed during 2024/25
| National Audit | Number of cases required | Number of cases submitted (percentage) |
| National audit of Falls (NAIF) Inpatient | No set of number required | 1 |
| POMH-UK topic 21b: The use of melatonin | No set of number required | 6 |
| POMH-UK topic 24a: Opioid medications in mental health service | No set of number required | 11 |
| POMH-UK topic 18c: Use of Clozapine | No set of number required | Data collection in progress |
| National Audit of Care at the End of Life (NACEL) Mental Health Spotlight Audit 2025 | No set of number required | Data collection in progress |
| National Audit of Eating Disorders (NAED) 2024/27 | No set of number required | Data collection in progress |
| National Confidential Enquiries | Number of cases required | Number of cases submitted (percentage) |
| Mental Health Clinical Outcome Review Programme – National Confidential Inquiry into Suicide and Homicide by People with Mental Illness | No set of number required | 18 |
| Learning Disabilities Mortality Review (LeDeR) | No set of number required | 14 |
The findings of three national clinical audits registered in the previous financial year(s) were reviewed by the provider in 2024/25 and LYPFT intends to take the following actions to improve the quality of healthcare provided:
Table three – findings of three national clinical audits registered in the previous financial year(s).
| National Audit | LYPFT action 2024/25 |
| National Clinical Audit of Psychosis (NCAP) 2023/24 – Early Intervention (EI) | The Service has begun work to ultimately gain a more accurate, continuous understanding of the NCAP data on a month-by-month basis. This will include embedding the use of and reporting around national codes. Once established, this will inform progress against the standards, monthly, over the year and allow for action to address areas of improvement in a timelier manner. Ongoing discussions with the Integrated Care Board (ICB) around appropriate levels of funding for service in order to meet the demands of EI work across the city will help to frame Service’s current performance. |
| POMH-UK Topic 22a: Use of anticholinergic (antimuscarinic) medicines in old age mental health services | A Quality Improvement project has been agreed within Pharmacy Services and Older People Services in order to improve areas of low compliance highlighted by the national project: documentation reviewing side effects in service users prescribed medications. |
| National audit of Dementia – spotlight (Memory Services) | The results of the project around access time and time for a diagnosis would feed into a larger piece of work reviewing the memory pathway scheduled for next financial year. |
Trust and Local Clinical Audit
This section is divided into two parts: Trustwide (part of the priority programme) and service/team clinical audits (local).
Table four – Number of clinical audits.
| Number of clinical audits | Trustwide | Service / Team |
| Registered during 2024/25 | 6 | 45 |
| Completed during 2024/25 | 5 | 41 |
Trust Clinical Audit
Trustwide clinical audits are part of the priority programme. They fulfil the criteria of high risk or high-profile projects identified by Trust management or Trustwide Clinical Governance. The completed Trustwide clinical audits are listed below alongside the actions to improve care:
Table five – Number of Trust clinical audits.
| Title | LYPFT actions |
| Audit of Observation and Engagement within inpatient settings at LYPFT | Findings to be disseminated across relevant Clinical Governance Groups and develop local actions: a) to raise the awareness and uptake of Therapeutic Observation training and competency assessments; b) to identify other local areas for improvement such as documentation or evidence of therapeutic engagement. |
| Medical Record Keeping Clinical Audit (baseline and re-audit) | Each clinician to review their own practice focusing in the following areas of low compliance: a) review of Psychotropic medications, b) recording information about Non-psychotropic medication (i.e. name, dose, and route of administration), c) stating allergy status, d) recording legal status and e) actions for service users and carers. |
| The application of mental state examination (MSE) to nursing documentation | Development of a training package on MSE to support the development of nursing staff skills/confidence. Development of a tool which amalgamates the MSE and 4c’s of documentation which provides guidance to clinical staff. Development of gold standard examples which can be incorporated in the training and guidance tool. |
| Memory Service National accreditation programme (MSNAP) | Service user to be informed of who will do assessment and post diagnostic session. Share assessments that documents risk with relevant GP. Create leaflet including service user’s awareness of rights to consent to treatment, access advocacy services, 2nd opinion, interpreting services, view records and raise complaints. Liaise with Estates to try to solve the issues with the soundproof of some clinical rooms and implement alarm system. Changed wording in assessment to show what care plan was as service do not have written care plans. Devise an induction timetable for new staff to inform staff who they will meet and what tasks they will undertake. |
The following Trust-wide clinical audit projects are in progress:
- Antimicrobial audit
- Triangle of care (re-audit)
- Trust wide Care Planning
- Multi-agency public protection arrangements (MAPPA)
- Re-audit of the application of mental state examination to nursing documentation
Local Clinical Audit
The reports of 41 completed local clinical audits were reviewed by the provider in 2024/25 and the Trust intends to take the following actions to improve the quality of healthcare provided (the below table highlights key themes and summarised quality improvement actions using the 6 domains of the STEEEP Models as part of the Trust Quality Strategic Plan):
Table six – Key themes and summarised quality improvement actions using the 6 domains of the STEEEP Models as part of the Trust Quality Strategic Plan.
| Audit Themes | Key quality improvement actions |
| Safety | To raise awareness among team members about NICE guidelines for management of behavioural and psychological symptoms of dementia (BPSD) among dementia service users. To reiterate the importance of non-pharmacological techniques of managing BPSD. At the same time to discuss the side effect of medications that are used in managing BPSD, specifically the risk of falls while using Benzodiazepines and cardiovascular risk while using antipsychotics. To improve the way in which the Shared Care guidance is communicated in the letters to the GP as it is difficult to determine who had had a significant increase in blood pressure or significant loss of weight given that the parameters are not communicated explicitly. Designate Follow-Up Champions: Assign team members to oversee Prolactin monitoring adherence, especially for service users on high-risk medications. This can be added to the monthly Key Performance Indicators (KPIs) overseen by physical health monitoring lead Providing accessible information about monitoring to all PICU staff both in full and in easy read format. Posters placed in doctor’s office and multi-disciplinary team (MDT) office to remind doctors to take these bloods as well as documenting if refused alongside the plan to re attempt. |
| Timely | Collaboration with diagnostic services will be enhanced to expedite neuroimaging processes and mitigate appointment rescheduling issues, thus reducing diagnostic delays. Also, documentation practices will be strengthened to clearly identify reasons for delays, enabling targeted interventions and continuous improvement efforts. In order to ensure that medication is regularly reviewed, any member of the team prescribing any anxiolytic or hypnotic medication should set a duration of 4 weeks. Any plan made to reduce and/or stop the medication should be documented both in the comments section of Electronic Prescribing and Medicines Administration (EPMA) and as a case note on Patient Record system. The delay in completed T3’s being sent to the Mental Health Legislation Team will be escalated to the CQC as this is potentially leading to unnecessary completion of Section 62’s. We propose creating a team approach of sending out 2-month ECT completion email and uploading response in Patient Record System rather than relying on one member of staff. Implement Reminder Systems: add prompts for Prolactin checks in GP letters to encourage timely six-month and annual follow-ups. |
| Effective | Discussion in MDT about starting medication especially anti-psychotics for BPSD. Any deviation from the NICE guidelines to be discussed in the MDT as well as service users/family members before starting treatment. To consider further training for the staff within this service to understand the connection between this medication group and gambling disorders. If the team had a greater understanding of the link, they would be more likely to recognise the importance of an accurate drug history and appropriate escalation. To introduce an ‘ACB score’ section in the initial assessment proforma and follow-up proforma templates as a prompt for checking for anticholinergic burden to alert clinicians when obtaining medication history and displaying easy-read posters in key areas as a prompt for clinicians. Provide clarification of the minimum documentation requirements for capacity assessments and best interest decision making for doctors within the service. This will be integrated into the induction process for new doctors and also distributed internally. To standardize documentation and protocols for documenting and acting on abnormal results to ensure consistency. |
| Efficient | Liaise with physical health leads to create an online daily updated shared check list to monitor compliance with the ECG completion and documentation standards. Streamlining of processes for documentation, with individualised care plans uploaded to the Patient Record System for ease of access and utilisation and the team no longer using patient shared drives. Service users to sign copies of their care plans and these can be uploaded onto the system. To develop a draft Weight Monitoring ‘Care Plan’ for Service Users prescribed a new Atypical Antipsychotic, with Nursing input. In order to prompt discussion of admitted service users in MDT, a new ‘Admissions’ section will be added to the existing MDT proforma. A note can also be added to the bottom of the document reminding those who complete the proforma to save this to the shared drive to ensure MDT documentation is accurately and consistently stored. On a case-by-case basis, we will also review each service user’s GP location and consider if it is appropriate to re-register them with a GP local to the Newsam Centre (for example, if they are having a long admission and require ongoing care from their GP). |
| Equitable | To ensure all service users prescribed specific medications (Clozapine and Lithium) have relevant care plans in place using care plan template guidance. Develop guidance for incorporating Positive Behavioural Support (PBS) language in to care plans and support relevant professionals in utilising the guidance when writing care plans. Improve service user’s involvement and co-production of PBS plans. Admission bloods to be added to the handover log to make sure these are offered to all service users again if they refuse the first time. To look at creating, with support from health facilitation, an easy read, accessible document to help explain the impact of antipsychotics on service users’ health, including potential side effects such as weight gain. |
| Patient Centred | To raise awareness of the resources available with accessible written information regarding medications for service users, both to service users and their families and to the Psychiatry team. Prior to the prescription of any anxiolytic or hypnotic medication, the potential risk of tolerance/dependence and therefore the intention of short-term use only should be explained to the service user, and the discussion documented clearly in the case note from that encounter. To have the easy-read information co-reviewed by service users with learning disabilities, to ensure it portrays the information in a clear and useful manner. Improve ward procedure around the sharing of PBS plans with young people and ensure accurate documentation of professional and young person familiarity of the plan. Safeguarding team to make it explicit to staff when providing advice, that they need to obtain the service user’s views and wishes, if not done so already, and to ensure this is recorded accurately by staff/safeguarding team, as evidence it has been completed. Enhance service user’s education: to inform service user on Hyperprolactinemia symptoms and the importance of monitoring to improve compliance and symptom reporting. |
Clinical Research
Clinical Research
- In 2024-25, the number of Trust service users, carers and staff recruited to participate in research approved by a research ethics committee was 275.
- 39 research studies across 15 clinical services were active during this period.
- The Research and Development Department received £1.4 million grant income during this period.
Participant Research Experience Survey
The Trust has been gathering feedback from research participants via the Participant Research Experience Survey since 2019. The NIHR Research Delivery Network developed this national survey to explore people’s experience of taking part in research in England. The responses are used to identify ways to improve people’s experience of research and to highlight areas that are working well. In LYPFT we use the feedback to check whether there is anything we can do locally to improve how we engage our participants.
We received 29 survey replies in 2024-25 with lots of good feedback about people’s experience of being involved in research alongside suggestions around ways to improve.
The following responses were in relation to the question ‘what was positive about taking part in the research’?
The knowledge the team had about diabetes and mental health was beneficial to me.
Learnt about staying positive and how to change certain situations.
Receiving intervention, lot of good advice and encouragement. Found coaching helpful.
Efficient and effective communication. Excellent people skills. Had someone to talk to.
The staff member I interacted with was always prompt at replying to any written communication. They showed empathy and patience during our check-ups and would send me reminders via other communication methods as I had said I forgot to routinely check emails.
The following feedback was given in response to the question ‘What would have made your research experience better?
Meet up after study finishes, keeping in touch.
Ability to get my results (i.e. was I taking a placebo or active medication) without going to GP (GP inaccessible & hard to get appointment).
Spend less time in the interview.
A more local experience.
I cannot think of any ways that the experience could be improved while maintaining the efficacy of the study.
Commissioning for Quality and Innovation (CQUIN)
The mandatory CQUIN scheme has been paused by NHS England, therefore there is no requirement to report this information in 2024-25.
National Quality Requirements
72-hour follow-up and readmissions
The percentage of patients who were followed up within 72 hours following discharge from inpatient care during the reporting period.
We currently have a standard of 80% for patients to receive a follow up review within 72 hours of discharge from inpatient services.
Table seven – The table below shows the percentage we achieved for each quarter.
| Year | Quarter one | Quarter two | Quarter three | Quarter four |
| 2024/2025 | 84.68% | 80.25% | 81.06% | 82.19% |
Our organisation considers that this percentage is as described for the following reasons:
- Our organisation routinely monitors performance and data quality for this metric to ensure that teams can fulfil the follow up target.
The organisation intends to take/has taken the following actions to improve the percentage, and so the quality of its services:
- Our organisation continues to maintain support with interpretation of requirements to ensure they are understood, and performance is properly captured.
- Our organisation will continue to monitor performance for follow up within 72 hours to ensure that people are followed up as quickly as possible post discharge.
- Our organisation will continue the high level of scrutiny of performance and recording for this metric to ensure that service users are followed up appropriately.
The percentage of patients aged: (i) 0 to 15 and (ii) 16 or over, readmitted to a hospital which forms part of the Trust within 28 days of being discharged from a hospital which forms part of the trust during the reporting period is shown in table eight.
Table eight
| Patients aged | Quarter one: discharges | Quarter one: readmission in 28 days | Quarter one: readmission rate |
| 0 to 15 | 4 | 1 | 25.0% |
| 16 plus | 374 | 7 | 1.9% |
| Summary | 378 | 8 | 2.1% |
| Patients aged | Quarter two: discharges | Quarter two: readmission in 28 days | Quarter two: readmission rate |
| 0 to 15 | 3 | 0 | 0.0% |
| 16 plus | 372 | 5 | 1.3% |
| Summary | 375 | 5 | 1.3% |
| Patients aged | Quarter three: discharges | Quarter three: readmission in 28 days | Quarter three: readmission rate |
| 0 to 15 | 4 | 0 | 0.0% |
| 16 plus | 374 | 6 | 1.6% |
| Summary | 378 | 6 | 1.6% |
| Patients aged | Quarter four: discharges | Quarter four: readmission in 28 days | Quarter four: readmission rate |
| 0 to 15 | 4 | 0 | 0.0% |
| 16 plus | 382 | 5 | 1.3% |
| Summary | 386 | 5 | 1.3% |
| Patients aged | Total discharges | Total readmission in 28 days | Total readmission rate |
| 0 to 15 | 15 | 1 | 6.7% |
| 16 plus | 1,502 | 23 | 1.5% |
| Summary | 1,517 | 24 | 1.6% |
Our organisation considers that this percentage is as described for the following reasons:
- The data is produced routinely following the agreed specification.
Our organisation intends to take/has taken the following actions to improve the percentage, and so the quality of its services:
- Readmissions are included within routine inpatient information sent to our inpatient services for their review.
The percentage of patients under 16 years old admitted to adult facilities:
- There were none during the reporting year of 2024/2025.
The percentage of admissions to acute wards for which the Crisis Resolution Home Treatment Team acted as a gatekeeper during the reporting period. Please note, this measure is no longer a requirement for the Quality Account.
Staff Survey

Thursday 13 March marked the national publication of the 2024 NHS Staff Survey results, as the Survey is officially classified as a national statistic.
64.46% of LYPFT staff said that if a friend or relative needed treatment, they would be happy with the standard of care provided by the organisation. The national average for this question was 64.84%.
We want teams to remain at the heart of shaping our Trust as a great place to work. To support this, we have compiled resources to help with Intention Planning, ensuring that results lead to meaningful action.
Community Mental Health Services 2024 Survey results
The National Service User Survey (NPS) programme was introduced in 2001 by the Department of Health, and subsequently moved to the Healthcare Commission, and then to the Care Quality Commission in April 2009. The results of the most recent Community Mental Health Services 2024 survey were published on 04th April 2025.
The results of the survey showed that Leeds and York Partnership NHS Foundation Trust are predominantly better than the sector scores.
Our highest scores were achieved for the following questions:
- Thinking about the last time you received therapy; did you have enough privacy to talk comfortably?
- Did your NHS mental health team treat you with care and compassion?
- Would you know who to contact out of office hours within the NHS if you had a crisis?
- Have any of the following been discussed with you about your medication? Purpose of medication
- Overall, in the last 12 months, did you feel that you were treated with respect and dignity by NHS mental health services?
Our lowest scoring results were in the following questions:
- In the last 12 months, did your NHS mental health team give you any help or advice with finding support for… Finding or keeping work
- In the last 12 months, did your NHS mental health team give you any help or advice with finding support for… Cost of living
- Aside from this questionnaire, in the last 12 months, have you been asked by NHS mental health services to give your views on the quality of your care?
- In the last 12 months, did your NHS mental health team give you any help or advice with finding support for… Financial advice or benefits
- Has your NHS mental health team asked if you need support to access your care and treatment?
These results have just been published at the time of writing this report. The Patient Carer and Experience Lead will coordinate an action plan in response to the results and support the relevant clinical teams to take the required action forward.
Care Quality Commission (CQC) Regulation, Ratings, and Improvement Plan
![]() Our organisation is required to register with the Care Quality Commission (CQC) and its current registration status is full registration without condition. The current overall rating achieved in December 2019 following inspection in July and August 2019 is good.
Our organisation is required to register with the Care Quality Commission (CQC) and its current registration status is full registration without condition. The current overall rating achieved in December 2019 following inspection in July and August 2019 is good.
As an organisation, we are registered with the CQC to carry out the following regulated activities:
- Treatment of disease, disorder, or injury.
- Assessment or medical treatment for persons detained under the Mental Health Act 1983.
- Diagnostic and screening procedures.
- Nursing care and personal care.
Leeds and York Partnership NHS Foundation Trust has not participated in any special reviews by the CQC during the reporting period .
The CQC currently inspect NHS organisations, using the five key questions. These are: Safe, Effective, Caring, Responsive, and Well led.
Our overall ratings are “good” for well led, effective, caring, and responsive. Our overall rating for “safe” is requires improvement.
In September 2024, our Mother and Baby Unit were inspected by CQC for the first time and achieved an overall rating of good.
In July 2024 CQC our Child and Adolescent Mental Health Services were inspected by CQC, and we are awaiting the report.
Change to the landscape of CQC inspections
In 2021, the CQC published its new strategy for Health and Social Care setting out changes to the way they regulate. From February 2024 the CQC started assessing all providers using a single assessment framework.
On the 15th of October 2024, Sir Mike Richards published a review of the CQC’s single assessment framework and its implementation, and on the 17th of October 2024, Dr Penelope Dash published an independent report focusing on the operational effectiveness of the CQC.
Both reviews concluded that there had been “significant failings in the internal workings of CQC.
CQC have accepted the high-level recommendations from both reviews and are taking rapid action in response.
The Regulation Team will keep abreast of any changes in CQC methodology through engagement events, CQC bulletin updates, the CQC Network Forum and are engaged with the CQC Regulatory Approach Advisory Group.
Information Governance
Our organisation completes an annual self-assessment against the NHS Digital Data Security & Protection Toolkit. The Toolkit is an online self-assessment tool that allows organisations to measure their performance against published standards. For the 2024-2025 reporting year the Toolkit has been completely revised and is now aligned to the Cyber Assessment Framework.
All organisations that have access to NHS patient data and systems must use the Toolkit to provide assurance that they are practising good data security, and that personal information is handled correctly.
Our organisation reported a position of ‘Standards Met’ on 30th June 2024, with all Compulsory Assertions completed by the June deadline. This was supported by an internal audit aligned to the NHS England National Audit Framework, with an outcome of “High Assurance” against the 10 National Data Guardian Standards. We were very pleased to receive an audit report without any improvement recommendations.
Work is underway on the 2024-2025 Data Security and Protection Toolkit reporting cycle, with a deadline of 30th June, and an internal audit scheduled for May 2025.
Additional Workstreams
Throughout the year our organisation has worked on several key Information Governance workstreams, including:
- Continuing to deliver Information Governance sign-off swiftly for new solutions, and to ensure that Information Governance / Data Protection due diligence upholds the principle of ‘Data Protection by Design and by Default’ when new solutions are considered or implemented, via a robust check and challenge / Data Protection Impact Assessment approach. This means that when our organisation implements new systems or processes, we ensure the safety and security of information is upheld.
- Servicing Data Protection Act Subject Access Requests against the statutory 1 calendar month timescale, with compliance at over 96% over the last 12 months. A Subject Access Request gives individuals the right to obtain a copy of their personal data, as well as other additional information. It helps people to understand how and why we are using their data, and check we are doing it lawfully.
- Maintaining our exemplary record of statutory compliance in our Freedom of Information Act request processing, with 100% of requests processed on time in the financial year to date. The Freedom of Information Act creates a general right of access to all types of recorded information held by most UK public authorities.
- Continuing to work to the revised NHS Digital Information Governance breach reporting standards, aligned to the UK General Data Protection Regulation / Data Protection Act 2018.
- Delivering high levels of clinical coding accuracy for Inpatient Finished Consultant Episodes, with an external audit confirming accuracy standards of 94% for Primary Diagnosis and 91.4% for Secondary Diagnosis.
- Enabling 24/7 availability of our medical records by breaking the reliance on paper records with the roll-out of digitised records stored in the MediViewer solution, presenting paper records digitally. MediViewer is now business-as-usual across the Trust, providing paper-lite care in all services.
- Implementing numerous data quality / data completeness workstreams, aiming to improve data quality and completeness standards throughout our organisation.
Payment by Results
Our organisation was not subject to the Payments by Results clinical coding audit during 2024/25 by the audit commission.
Learning from Deaths
Our organisation continues to review all deaths of service users that have been in receipt of care by our organisation at the time of their death or within 6-months since their discharge from our care. This is in accordance with the Learning from Deaths Policy. During 2024 we revised our Learning from Deaths policy to conform with the Royal College of Psychiatry guidance.
All deaths that are either reported on the Trust incident reporting system or identified from data taken from the NHS Spine and cross referenced with Care Director receive an initial review of a service user’s involvement with LYPFT. Where a death is identified as being in scope for further review, either under the Trust’s Learning From Deaths policy or the Patient Safety Incident Investigation Framework policy, a table top review of care provided is completed and if it is identified that there is the potential for learning then a learning review (like an investigation) will take place to identify where our organisation can improve.
Summary of 2024-2025
During 2024/2025, 205 of Leeds and York Partnership NHS Foundation Trusts patient deaths were recorded on Datix (the Trusts risk management information system). In addition, we also reviewed 865 deaths which were identified from data taken from the NHS Spine and then cross referenced with Care Director (our organisation’s electronic care records system). These cases were reviewed to consider if any further action was required and if these could provide opportunities for learning. Overall, a total of 1070 deaths were reviewed in our organisation in 2024/25, compared to the 2023/24 Quality Accounts when 1391 were reviewed.
All deaths reported are reviewed due to the individual having had some form of contact with Mental Health & Learning Disability services, which may have ranged from an initial assessment in A&E (Accident & Emergency) to full care co-ordination or admission as an inpatient, some of these deaths will have had a one-off assessment and no further contact with any of our services. Others will have accessed an increased range of services or more intensive, consistent contact. The initial review of the death considers information such as interventions from Mental Health & Learning Disability services in association with the cause of death.
Of those 1070 deaths, 15 deaths were reported to StEIS (NHS England Strategic Executive Information System). Of those incidents 9 were reported as per the Serious Incident (SI) Framework (March 2015) and 6 were reported as per the Patient Safety Incident Reporting Framework (PSIRF). The SI framework was be replaced by the Patient Safety Incident Reporting Framework (PSIRF) in July 2024.
The investigation process enables us to identify learning, learn lessons and improve care and treatment in the future.
A further 91 deaths had further review such as Structured Judgement Review, After Action Review, Specialist Thematic Review or Concise Investigation.
The number of deaths reported on Datix, and those progressed to a further investigation are detailed in table 9 below per quarter for 2024-2025.
Table nine
Please note that LIMM stands for Learning from Incidents and Mortality.
| Financial quarter | Deaths reported from NHS Spine | Deaths reported on DATIX | Total Deaths reviewed by Patient Safety Team | Deaths subject to discussion at LIMM | Number of deaths progressed to After Action Review, STR or Concise | Number progressed to SJR | Number of deaths investigated as a Serious Incident and reported on STEIS |
| Quarter 1 Apr – Jun 2024 |
224 | 54 | 278 | 38 | 1 | 2 | 9 |
| Quarter 2 Jul – Sept 2024 |
185 | 67 | 252 | 53 | 3 | 13 | 2 |
| Quarter 3 Oct – Dec 2024 |
217 | 54 | 271 | 42 | 3 | 6 | 2 |
| Quarter 4 Jan – Mar 2025 |
239 | 30 | 269 | 24 | 5 | 43 | 2 |
| Total | 865 | 205 | 1070 | 157 | 12 | 64 | 15 |
This report details how many deaths, extracted using date the death was reported to Datix, this includes deaths from natural causes as well as deaths meeting the LFPSE definition of a death.
There are currently two investigations in relation to deaths which were commissioned in 2023-24 and 11 from 2024-2025 which are in progress and will be carried over into 2025-26. For 2024-25 where the full Serious Incident investigation process or the Patient Safety Incident Investigation process has not been completed, we cannot determine at this stage if there are any of elements of learning from the care delivered in our organisation. The findings of these 13 reports will be reported in the bi-annual Learning from Death Reports and the Quality Account submission for 2025-26.
Of the deaths reviewed during the reporting period 2024-2025, two are estimated to be more likely than not to have been due to problems in the care provided to the service user. Both of these incidents remain in the review process at time of writing and therefore full findings are not yet available to share.
Table 10 – Deaths reviewed/ investigated found to be due to problems in care by quarter.
| Financial Quarters (2024-2025) | Deaths reviewed/ investigated found to be due to problems in care |
| Quarter 1, Apr – Jun 2024 | 0% |
| Quarter 2, Jul – Sept 2024 | 0% |
| Quarter 3, Oct – Dec 2024 | 0.36% (1 death out of 271 reviewed) |
| Quarter 4, Jan – Mar 2025 | 3.37% (1 death out of 269 reviewed) |
| Total | 0.18% (2 deaths out of 1070 reported) |
These numbers have been estimated using the Trusts incident reporting system, the initial findings from the tabletop reviews and findings from completed serious incident reviews. Both of these incidents occurred post transition to PSIRF and are being reviewed through a Patient Safey Incident Investigation. Once completed findings will be shared in the bi-annual Learning from Death Reports and the Quality Account submission for 2025-26.
There have been six investigations completed after 1st April 2024 which related to deaths which took place before the start of the reporting period. Three relate to deaths that occurred in the 2022-2023 financial year, and three relate to deaths that occurred in the reporting year 2023-2024.
Three of the deaths for the reporting period 2022-2023 (representing 2.09% of the 143 deaths for this reporting period) and one from the reporting period 2023-2024 (representing 0.33% of the 297 deaths for this reporting period) are judged to be more likely than not to have been due to problems in the care provided to the patient. This number has been estimated using the Trusts incident reporting system and serious incident review process.
The detail of the learning is summarised in Table 11 below.
Table 11 – Summary of what the organisation has learnt from deaths judged to be more likely than not to have been due to problems in the care provided.
| Summary of each death where it was judged to be more likely than not to have been due to problems in the care provided. | Description of actions taken and learning as a result of the investigation. | What has been the impact of the actions taken? |
| A staff member was delegated to duties with service users before receiving a handover or a ward induction. There was also a lack of provision of psychological practitioners on the ward which meant the staff team were not adequately supported to uphold a psychologically informed, case formulation led approach to practice. This is necessary for working with someone with trauma based emotional and relational difficulties associated with a ‘personality disorder’ diagnosis. |
Our organisation has now developed a clear induction process for bank and agency staff which includes comprehensive handovers prior to being delegated patient facing duties.
A review of workforce development was undertaken to support recruitment to psychological professions. A business continuity/contingency management plan was developed to manage vacancy/absence related gaps in psychology provision. |
Changes to the induction process have been taken through local level Clinical Governance meetings and bank staff forums and updates have been made to the Standard Operating Procedure. The changes are now embedded within teams.
Additional psychology practitioners have been recruited and if urgent gaps in psychology provision are identified there is now a standardised process to review the impact of the gaps and consider available resource within LYPFT and external, such as agency to meet urgent needs. |
| Documentational issues led to a CMHT team being unaware of recent crisis contacts. There were also missed opportunities to provide a more robust risk assessment and subsequent safety planning as a result of standardised triage templates not being used. Staff involved were bank and agency staff members who had not received a service specific induction. | The team has now developed a clear induction process for bank and agency staff. This includes a sub section for new starters within the teams standard operating procedure to highlight key tools used to standardise practice. A regular audit process was implemented to review the quality of triages and ensure swift action should it be identified that standardised triage templates were not being utilised. | Changes to the induction process have been taken through local level Clinical Governance meetings and bank staff forums and updates have been made to the Standard Operating Procedure. The changes are now embedded within teams. |
| There was a lack of formal capacity assessment documented alongside insufficient scrutiny and engagement with the service user prior to leaving the ward. There was a lack of engagement with the service user’s family around leave and any associated risks or concerns. There was also a lack of Trust awareness and guidance on the exploration of risk and risk management strategies in relation to internet use/social media. | An anonymised case study of this incident has been included in the level 2 mental capacity training when discussing consent processes. The systems and processes handbook was reviewed and updated to outline expectations around leave and discharge processes for service users. This included expectations relating to risk assessment, safety planning and involvement of families. Recurrent bitesize training was developed and delivered to all band 6 staff in the service line, with a plan for these staff to disseminate further within their teams as a regular refresher to cover the rights of informal patients alongside risk assessment and safety planning. A Patient Information leaflet was developed to ensure informal patients understand their rights and the expectations of admission. | All of these changes have been completed, embedded, and shared at unified clinical governance to ensure other service lines are able to benefit from the changes made. |
| There was a delay in identifying a named key worker and a delay in booking a medical appointment for the service user. Safeguarding concerns were also noted but did not. | A new process was developed to ensure that all individuals requiring a medical appointment are booked in on the same day. Any delays are escalated via an agreed escalation process. A new process was developed to ensure that key workers are allocated within 72 hours of referral and any delays are escalated via an agreed process. | The changes are now embedded within the team and have been shared at clinical governance forums. |
Our organisation considers that this data is as described for the following reasons:
- The organisation does not rely solely on Datix reporting of deaths but systematically searches for any deaths of people known to its services through the NHS Spine.
- The organisation has a multi-professional group which considers all these deaths, to determine which deaths need further investigation or review.
- The organisation provides training in how to undertake SJRs.
Our organisation has taken the following actions to improve, and so the quality of its services, by:
Our organisation actively encourages incident reporting and has developed a supportive and responsive workplace culture towards patient safety. Our organisation’s policy stipulates that all known deaths are reported via Datix (our electronic incident reporting system). Following the report of a death (or any harms of severe or death and occasionally moderate harm) on the Datix system, these are discussed within clinical governance forums and if appropriate, at our Learning from Incidents and Mortality Meeting. Our organisation produces a monthly summary report (CLIP – Complaints, Litigation, Incidents, Patient Advice & Liaison) to aid discussion and highlight any areas of concern. All learning disability patient deaths are subject to a review regardless of whether they are expected or unexpected deaths. This process is via the Learning Disabilities Mortality Review (LeDeR).
The bi-annual Learning from Deaths reports is a framework to help standardise and improve how NHS providers identify, report, investigate, and learn from deaths. From 2024-2025 the reports have highlighted several key areas of good practice and some opportunities for learning and improving. The learning is taken from completed concise and comprehensive incident reports. We have identified below some issues that have been identified throughout the past twelve months and the action taken to address these:
- One of the key themes from completed reviews within the reporting period 2024-2025 is issues in communication between services. Based on these findings, a work stream has been created between Leeds and York Partnership NHS Foundation Trust services and Forward Leeds to review and update the local working agreement, defining the roles and responsibilities of each team and communication expectations between the services to improve care delivery.
- A collaborative approach has been taken towards responding to patient safety incidents and sharing learning with partner organisations. In Q1 and Q2 2024/25, two joint comprehensive reviews took place between Leeds and York Partnership NHS Foundation Trust, Leeds Community Healthcare (LCH) and Community Links in response to deaths. Both reviews led to the development of standard operating procedures between the Leeds and York Partnership NHS Foundation Trust Patient Safety Team and that of these services in respect of reviewing incidents and sharing learning.
- There was a theme noted of service users being referred to a Leeds and York Partnership NHS Foundation Trust service and then discharged due to lack of response or engagement, without the service user being assessed or spoken to. Following a review of the process within the service, referrals are no longer being left open for call backs, information is gathered through triage and any plans for assessment are agreed with the professional at the point of referral with clinical decision making documented in a standardised format to avoid delays in assessment.
- The Learning from Incidents and Mortality Meeting (LIMM) identified 40 deaths of service users in receipt of care or on the waiting list in the Gender ID Service between 2020 and 2024 (these are included within the chart on page 48). Whilst LIMM had completed an initial Datix review for each death, it was agreed after further discussion and identification that 8 deaths were by suicide, that a series of Structured Judgment Reviews (SJR’s) would be completed to determine any themes/trends and associated learning. A thematic review was completed and shared within the Trusts governance forums. An action plan was developed by the Service Line.
Training
We have delivered Structured Judgement Review Training to our staff throughout 2024-2025. Clinical Risk and Safety Planning training has also been delivered throughout this reporting period and will continue to be delivered throughout 2025-2026.
With the introduction of PSIRF in July 2024 three new training courses for staff facilitating After Action Reviews, Specialist Thematic Review and Patient Safety Incident Investigations. All three training courses were developed by the Patient Safety Team and have been delivered throughout 2024-2025, which will continue throughout 2025-2026.
Patient Safety Partners
The Patient Safety Partner (PSP) is a new and evolving role developed by NHS England / Improvement as part of the NHS Patient Safety Strategy (July 2019) to help improve patient safety across the NHS in the UK. Within our organisation, we are welcoming PSPs to offer support alongside our staff, patients, families/carers to influence and improve safety across our range of services. PSPs can be patients, carers, family members or other lay and this offers a great opportunity to share interests, experiences, and skills to help develop the new PSP role and be a part of our team.
The organisation will be looking to embed these roles within the next financial year.
Patient Safety Newsletter
The Patient Safety Newsletter has continued with quarterly publications. This includes any recent information relating to all patient safety matters, provides details on the training for PSIRF learning reviews and shares learning from completed learning reviews across the organisation.
Patient Safety Incidents
Learn from Patient Safety Events (LFPSE) is a system managed by NHS England and NHS Improvement and is the single national NHS system for recording patient safety events. A patient safety event is any unintended or unexpected incident that could have or did lead to harm for one or more patients receiving healthcare. LFPSE is a centralised system to record and analyse information. Providers are able to see overviews of reporting within their own organisation and within other organisations. It is hoped that this will allow for more effective learning from events, with patient safety improving.
In 2025/2026 we will be progressing action to validate, and quality check the submissions we make to LFPSE.
Inquests
Between the 1 April 2024 and 31 March 2025 we were registered by the coroner to be involved in 28 inquests, with our staff providing statements and attending in person as required.
From these inquests, our organisation received nil Prevention of Future Death (PFD) reports which are served by the Coroner under the Coroner’s (investigations) Regulation 28.
Section Three
Improving the Quality of Our Services
This next section of the Quality Account is an opportunity for us to share some of the important work we have done over the year and celebrate our achievements.
We have continued to deliver on our core ambition to support our service users and carers, our staff, and the communities we serve to live healthy and fulfilling lives.
As part of the work in developing this section of the Quality Account, we have consulted with a group of service users and carers on the content of the document to provide feedback on what they would like to see, and how the document can be improved to make it more accessible and easier to read.
Feedback included:
They felt it was important to use plain language. Keeping it simple. Keeping the report relevant and concise.
Examples of the impact quality changes had on service users to humanise the work and understand different aspects of people’s experience. This could help show the work in context.
They would like more explanation in the PALS section about what went wrong when concerns were raised and what was done about it, with some anonymised examples of learning. More explanation of what were the clinical treatments that went wrong. How many complaints were upheld, and how this reflects the services’ ability to learn and improve based on the feedback.
They thought some inclusion regarding how well partnership work is progressing would be useful.
The inclusion of some information on waiting lists and what we are doing about them e.g. transformation work in the community and plans to address ADHD assessment waiting lists.
Changes have been made to the Quality Account on the basis of this feedback with some comments being held to assist in the development of the 2025/2026 Quality Account.
Community Mental Health Transformation
 Community mental health care and support in Leeds is changing, with all areas of the city now benefiting from transformed services.
Community mental health care and support in Leeds is changing, with all areas of the city now benefiting from transformed services.
From March 2025, all areas of Leeds will be served by mental health teams made up of people from different health, social and voluntary organisations.
By bringing services together, people in Leeds living with mental and emotional health difficulties will experience more joined up community mental health services and support, providing them with easier access to the expertise and care they need.
Initial changes will focus on how members of these teams work together, how patients are triaged, and securing access to advice and guidance on psychological therapies. Over time, keyworkers will also be introduced so that everyone who is getting community mental health care from the team will have a dedicated, named contact to help them on their journey.
Together, these changes will help us to remove the barriers that may stop people in Leeds from getting the mental health care and support they need, so that they can continue to live as well as possible in the community.
A new approach to patient safety
 Patient safety is the guiding principle of the NHS and we have always been committed to doing everything we can to keep people safe while they are receiving care from our Trust.
Patient safety is the guiding principle of the NHS and we have always been committed to doing everything we can to keep people safe while they are receiving care from our Trust.
In recent years there’s been a real shift in the way the NHS thinks about patient safety, and the way we should react and learn when things go wrong.
In 2024, we adopted and rolled out what is known as PSIRF – the Patient Safety Incident Response Framework – which is a key part of the NHS Patient Safety Strategy.
Put simply, it changes the way we respond to patient safety incidents.
Rather than requiring us to investigate all and only incidents that meet a specific set of criteria, under PSIRF we can choose to focus on the patient safety events that we know will provide us with the greatest opportunity to learn and improve.
There are many benefits to the new approach, which will allow us to respond proportionately to a patient safety event, while treating everyone involved fairly and with compassion.
Adult Eating Disorders Service CONNECT introduces groundbreaking referral criteria adjustment
 CONNECT, a specialised eating disorders service, launched a pilot programme in 2024 to update its referral criteria, ensuring greater access to care for individuals in need.
CONNECT, a specialised eating disorders service, launched a pilot programme in 2024 to update its referral criteria, ensuring greater access to care for individuals in need.
This significant adjustment, in line with the World Health Organisation’s ICD-11 standards, reflects a shift in diagnostic practices and demonstrates CONNECT’s commitment to prioritising patient wellbeing.
Traditionally, the CONNECT service has based its community referrals on a combination of core eating disorder behaviours, such as daily bingeing and purging, and body mass index (BMI) thresholds. BMI is a measurement of someone’s weight in relation to their height. However, many individuals experiencing anorexia with significant weight loss were excluded because their BMI remained within a ‘healthy’ range. Therefore, they were not able to receive the care they needed.
Under the pilot, which runs until June 2025, CONNECT will consider a 20% weight loss over the past six months, regardless of BMI, in addition to the existing criteria.
This change is a more nuanced approach that aligns our service with the expected standards from the World Health Organisation and allows us to provide treatment to individuals who previously would have been excluded because of strict BMI thresholds.
Our continued commitment to improving NHS care for veterans
 Leeds and York Partnership NHS Foundation Trust has been re-accredited as Veteran Aware in recognition of its commitment to improving NHS care for veterans, reservists, members of the armed forces and their families.
Leeds and York Partnership NHS Foundation Trust has been re-accredited as Veteran Aware in recognition of its commitment to improving NHS care for veterans, reservists, members of the armed forces and their families.
Leeds and York Partnership NHS Foundation Trust’s Veteran Aware accreditation comes from the Veterans Covenant Healthcare Alliance (VCHA) and was originally given to Leeds and York Partnership NHS Foundation Trust in 2021. Our organisation is part of a growing number of NHS Trusts gaining this accolade.
The re-accreditation acknowledges the Trust’s continued commitment to a number of key pledges, including:
- Ensuring that the armed forces community is never disadvantaged compared to other patients, in line with the NHS’s commitment to the Armed Forces Covenant,
- Training relevant staff on veteran specific culture or needs,
- Making veterans, reservists and service families aware of appropriate charities or NHS services beneficial to them, such as mental health services or support with financial and/or benefit claims, and
- Supporting the armed forces as an employer.
How co-production leads to positive practice at Red Kite View
 Our purpose-built Children And Young People’s Inpatient Mental Health Unit, Red Kite View, offers short-term intensive assessment and treatment for young people between the ages of 13-17 who can no longer be cared for in the community, or where their mental health needs mean they are unsafe in the community.
Our purpose-built Children And Young People’s Inpatient Mental Health Unit, Red Kite View, offers short-term intensive assessment and treatment for young people between the ages of 13-17 who can no longer be cared for in the community, or where their mental health needs mean they are unsafe in the community.
Since its initial development, co-production has been at the heart of Red Kite View; young people and their families with lived experience were involved in the design and development of the service, including a co-produced Red Kite View Charter.
On 1 May 2024, Red Kite View won the Children and Young People’s Mental Health Services (incl. Transition Services and those from 0-25) Award at the Positive Practice in Mental Health Awards (PPIMH). The work on co-production and following the service’s values demonstrates the commitment to positive practice, as do their clinical models and innovative care and treatment.
Since opening in 2022, Red Kite View has provided care closer to home and has continued to reduce the length of stay for young people.
Feel Good Mealtimes

The above infographic is an illustrated tray held by two hands displaying items associated with eating and drinking—such as a mug, spoon, oven mitt, and food packets—alongside key phrases: Culture and personal customs, Helping with the meal, Options for food and drink, Independence, Choking or coughing?, Eating, drinking, and swallowing skills, Support and social needs.
LYPFT’s Speech and Language Therapy and Research and Development teams are encouraging ward staff to make simple changes at mealtimes to improve mental wellbeing and support patient recovery.
The Me at Mealtimes study explored patient experiences and perspectives on mealtimes at Leeds and York Partnership NHS Foundation Trust. Patients and staff shared insights on making mealtimes more enjoyable and beneficial for mental wellbeing. Unfortunately, some patients found mealtimes stressful, anxiety-inducing, and noisy, highlighting the need for improvements.
The research concluded with a helpful framework – called C.H.O.I.C.E.S – which can be used to ask each person what’s important for them at mealtimes. The aim is to promote person-centred mealtimes by asking about the following topics.
- Culture and personal customs
- Helping with the meal – feeling involved
- Options for food and drink – considering where, when, what food, and who with?
- Independence – adapting institutional settings
- Choking or coughing? – recognising early warning signs
- Eating, drinking, and swallowing skills – listening to individual insights and concerns
- Support and social needs – addressing personal preferences and offering flexibility
Patients and staff at Asket Croft Rehabilitation Unit are now collaborating with Leeds and York Partnership NHS Foundation Trust Quality Improvement Team on the Feelgood Mealtimes Project, with a full evaluation of the study set to take place in summer 2025.
Patient and Carer Experience Team
Service User Network (SUN)
What is SUN?
![]() SUN is the Service User Network. It’s a group for people with lived experience of our organisation’s mental health and learning disability services – as service users or as relatives, friends or carers of service users.
SUN is the Service User Network. It’s a group for people with lived experience of our organisation’s mental health and learning disability services – as service users or as relatives, friends or carers of service users.
When is SUN?
SUN is held on the first Wednesday of every month and is held alternatively face to face and online. For details of how to join SUN – please email the Patient Experience Team.
Our thriving Service User Network (SUN) meets monthly and welcomes people with lived experience of our organisation’s mental health and learning disability services, either as someone who has accessed our services or as a relative, friend or carer of someone who has been supported by our services.The number of people attending SUN meetings is increasing month on month. 20+ SUN members routinely attend each meeting. 61 different members attended one or more SUN meetings during 2024 – 2025. SUN members have requested that the meetings are held online and face to face, on alternate months.
SUN meetings are co-chaired by Usmaan Khan and Carole Myers, lived experience partners, who plan the agenda for the meetings on behalf of the SUN members. SUN has hosted a wide range of activities and speakers over the past year. Each meeting gives people an opportunity to find out more about services or to get involved to help influence improvements to our mental health and learning disability services. The SUN is an inclusive group and welcomes people from a diverse range of backgrounds and ages.
SUN members gave their feedback relating to the following topics presented at SUN Meetings 2024-2025
- Developing a trauma-informed culture in Community Mental Health services
- Update LYPFT’s Quality Account
- Autism and ADHD priorities for Leeds
- Update from the Place Visits 2024
- NHS App & Mental Health Appointments
- Research and Development Team priorities
- PCREF
- LYPFT’s Brand Refresh Update
- Me and Mealtime Research
- Community Mental Health Transformation
- Shore Up Social Club
- LYPFT’s Risk Ax and Safety Planning Update
- LYPFT’s Health Equity Strategy
- LYPFT’s EMERGE Service – Complex and Emotional Needs
Involvement and Co Production Projects
189 SUN members are signed up to the SUN involvement distribution network which enables members to receive timely, up to date information linked to involvement opportunities across the Trust, at a Leeds, West Yorkshire and national level. Involvement opportunities are also shared among the Trust’s internal service user networks such as EMERGE, CONNECT, Rehab and Recovery, CREST, Forensic Services etc, demonstrating that involvement opportunities are shared with a diverse range of people.
The Patient, Carer and Experience Team (PCET) along with the help of the SUN co chairs have been successful over the past year in encouraging more people from diverse backgrounds to attend the SUN meetings and to get involved in involvement opportunities. SUN members can offer experiences and feedback from a wide range of perspectives including male/female, young person, older person, perinatal mental ill health, trauma, PTSD, emotional dysregulation, experience of being sectioned, neurodivergent, LGBTQ+ and ethnically diverse cultural backgrounds. A priority for the PCET over 2025/26 is to ensure we capture people’s demographics, so that we can evidence this.
During 2024/2025, 82 lived experience partners have been involved in 66 different involvement and co production projects and initiatives across the Trust.
Service users and carers have worked together with staff members to co-produce a plethora of projects and initiatives across the Trust.
The following projects are some examples which have been co-produced over the past year.
HSW Induction Workshops
Workshops covering what makes a positive experience for service users and the importance of carer awareness were co delivered by staff, service users and carers at three Health Support Worker induction programmes in June, July and October 2024. They are now an integral part of the HSW induction week.
Website Working Group
Two lived experience partners with special interests in digital and on-line accessibility have been welcomed as valued partners of the Trusts Website working group. They have been encouraged to raise queries and to make suggestions as to how the Trust websites can be made more accessible.
Patient and Carer Race Equity Framework Recruitment
The PCET has worked closely with the Clinical Inclusion Service Lead, who is leading on work linked to the Patient and Carer Race Equity Framework (PCREF) to recruit four lived experience partners who are from cultural minority backgrounds and have experience of being subjected to restrictive practice. They will form part of a PCREF advisory board. The PCET will continue to support work linked to PCREF.
Perinatal Mental Health Regional Collaborative – Co-production Group Induction event
A co-production group linked to the regional Perinatal Collaborative and a task group coordinated by the PCET is working to codesign an induction event which will include information on the NHS England transformation roadmap, information about the Mother and Baby Unit situated at The Mount and promote opportunities for mums and their partners to get involved to improve perinatal services.
Lived experience linked to Community Mental Health Transformation
In July 24 successful recruitment and interview arrangements were co-ordinated for the Focus Area steering group and Eating Distress sub-group, with four people appointed to lived experience roles. Publicity was also distributed widely to enable the setting up of the Neuro-diversity sub-group and focus groups.
Lived Experience Involvement on Recruitment Panels
Two lived experience partners were part of the Trusts Values Based Recruitment working group led by HR during the past year. To ensure Lived Experience Partners feel confident to be part of recruitment panels, the PCET co-produced an interviews skills workshop together with service users and carers and staff members from the Trust’s Recovery College. The workshop supports people to understand the Trusts values-based recruitment process and provides people with an opportunity to try out asking questions in a safe space. The workshop runs over two morning sessions.
Lived Experience Partners have been on recruitment panels for the following roles:
- Psychological Professions – Crisis Resolution Intensive Support Service (CRISS)
- Clinical Psychologist – Rehab and Recovery
- Practitioner- Leeds Autism Diagnostic Service
- Safeguarding Specialist Practitioner
- Clinical Psychologist-Working Age Adult Community Mental Health Team
- Assistant Psychologist – WAA Community Mental Health Team
- Consultant – Child and Adolescent Mental Health Services/ Red Kite View
- Consultant- Aspire
- Consultant – Learning Disability Service
- Consultant Psychiatrist – Forensic Inpatient Services
- Consultant Psychiatrist – Older Peoples Services
- Consultant Psychiatrist – Forward Leeds
Have Your Say – organisational feedback measure
Have Your Say is our organisations feedback measure which was co-produced with lived experience partners and staff members and includes the Friends and Family Test (FFT) question – What was your overall experience of our services? Have Your Say enables people (both service users and carers) to give us their feedback anonymously, about the care they have been provided with, at any point in their care journey. In trying to make the feedback measure accessible to all, we provide several ways in which people can give us their feedback.
People can complete postcards on our inpatient wards, there’s an online survey, a QR code which can be accessed using a mobile phone or tablet. There’s also an identified telephone number and an email address and a video has been made which interprets the questions into British Sign Language.
Table 13 below shows the number of people who have provided feedback over the past year and shows in percentages whether people said their overall experience of our services was positive, negative or people said it was OK or didn’t know.
Table 13 – Number of people who have provided feedback over the past year and experience.
| Month and year | Numbers of people who provided feedback | Positive rating of overall experience of care | OK/Don’t know rating of overall experience of care | Negative rating of overall experience of care |
| Apr 24 | 188 | 88% | 8% | 4% |
| May 24 | 194 | 87% | 8% | 5% |
| Jun 24 | 156 | 90% | 3% | 6% |
| Jul 24 | 215 | 88% | 5% | 7% |
| Aug 24 | 159 | 94% | 4% | 2% |
| Sept 24 | 160 | 90% | 7% | 3% |
| Oct 24 | 230 | 91% | 7% | 2% |
| Nov 24 | 185 | 88% | 9% | 3% |
| Dec 24 | 133 | 92% | 2% | 6% |
| Jan 25 | 201 | 90% | 7% | 3% |
| Feb 25 | 162 | 87% | 7% | 6% |
| Mar 25 | 136 | 91% | 6% | 3% |
Encouraging more people to give us their feedback
HYS drop-in sessions are held every other Friday in the Becklin Centre café area between 10.30am and 12pm. These sessions have helped to increase the numbers of feedback received for the Working Age Adult inpatient wards. The drop-in sessions are supported by a PCET member and volunteers from the Trusts Volunteer Service. Involving volunteers to help collect feedback from service users has been vital, as volunteers can spend quality time with service users, explaining that they are not staff members, and therefore giving service users the confidence to give their feedback freely, without worrying that their care may be affected. The volunteers report that supporting the HYS drop-in sessions gives them a sense of purpose and they hear from people, who may not usually be heard. The volunteers, who have experienced mental ill health in the past or are still in receipt of services, provide hope and inspiration to current inpatient service users, that recovery is possible and that they can go on to lead purposeful and meaningful lives.
In 2025/26 we plan to work closely with the IT team to enable services to send out a link to the HYS questions by text to service users.
Triangle of Care Champion Groups
 Triangle of Care champion meetings have continued to be held on a bi-monthly basis over the past year. The meeting is chaired by the PCET lead and upwards of 20 plus Triangle of Care champions attend the meeting on a regular basis. A representative from Carers Leeds attends the meeting ensuring that we have established a good working relationship with Carers Leeds, enabling us to work together to overcome any barriers to supporting and involving carers.
Triangle of Care champion meetings have continued to be held on a bi-monthly basis over the past year. The meeting is chaired by the PCET lead and upwards of 20 plus Triangle of Care champions attend the meeting on a regular basis. A representative from Carers Leeds attends the meeting ensuring that we have established a good working relationship with Carers Leeds, enabling us to work together to overcome any barriers to supporting and involving carers.
Board Stories
Board meetings are held in public and provide an opportunity for service users, carers, staff members and members of the public to attend the first part of the meeting, to raise any questions or concerns. On a bimonthly basis, lived experience partners are invited to talk to the Board members about their experience of our services and/or how they have been involved in service development. It’s a great way of highlighting the excellent involvement/learning from lived experience work that goes on in our organisation and often supports board members to think about discussions they have in other meetings across our organisation.
We have reflected on the stories told over the past year and it was acknowledged that over 24/25, the stories to the board have focused on lived experience partners using their experiences to get involved, to drive change across the organisation. For 2025/2026, board members have asked for a focus on people’s personal experiences and stories of being supported by the Trust’s services, to celebrate and highlight the great work which our staff members do, but equally to highlight experiences of care which have not gone so well, but learning has since taken place to introduce positive change.
Partnership Working – Working together with other organisations
 Leeds Carers Partnership (LCP) is a multi-agency partnership of staff and carers in health, social care and the voluntary sector and oversees delivery of the Leeds Carers Strategy 2020 – 2025 which has 6 main priorities. As a member, our organisation’s commitment to the Triangle of Care framework ensures we support the strategy’s priorities of improving the identification of carers and supporting carers to care.
Leeds Carers Partnership (LCP) is a multi-agency partnership of staff and carers in health, social care and the voluntary sector and oversees delivery of the Leeds Carers Strategy 2020 – 2025 which has 6 main priorities. As a member, our organisation’s commitment to the Triangle of Care framework ensures we support the strategy’s priorities of improving the identification of carers and supporting carers to care.
Carers and their essential role are identified at first contact with our services or as soon as possible afterward, ensuring that carers are aware of or referred to Carers Leeds or Leeds Young Carers Support Service to get support if required. Carers are also active members of our Service User Network and use their lived experience to influence change and innovation in the services that we provide.
Carers Leeds
Our Trust works closely with Carers Leeds to ensure that we are meaningfully involving and supporting our carers. Tom Harris, Training and Evaluation Team Leader at Carers Leeds regularly attends the Trusts bimonthly Triangle of Care Champions meeting which enables staff members to keep updated with resources and information they can share with unpaid carers.
Patient Voices Partnership (PVP)
The Patient and Carer Experience Team are members of the PVP. PVP is a group of passionate and motivated health and care professionals whose roles involve listening to people across the city. The group is led by Healthwatch and has the aim of putting people’s voices at the centre of all health and care decision making, with a particular focus on ensuring those who face the most inequalities to accessing health and care services, are listened to.
Celebrating Co-Production and Partnership Work: Inspiring Stories and Developments from the Trust
“It was an inspiring, stimulating, worthwhile, and truly uplifting afternoon” is some feedback we received after our Annual General Meeting and Improving Health and Lives Together, a celebration of our partnership work event.
We had exciting presentations from our service user groups and trust teams, where we shared what makes us an outstanding and inclusive Trust. There was also an opportunity for those attending to field questions.
The day offered the chance to learn about our services’ vital work, including the work with service users supporting co-production. It featured our AGM with updates from across the Trust from our Chair, Merran McRae, Chief Executive Sara Munro, Lead Governor Les France and Chief Financial Officer Dawn Hanwell.
In the afternoon, we welcome co-hosts Shaun Webster MBE, the Involvement Coordinator from our Learning Disability Services’ Involvement Team, and Oliver Tipper, the Head of Communications at Leeds and York Partnership NHS Foundation Trust. The Partnership Celebration Event 2024 featured presentations from our service user groups and trust teams.
We heard from:
- Working Together with Lived Experience Partners to co-design and co-deliver staff training: Health Care Support Worker Induction from the Practice Development Team.
- Creative Group Projects: Older People Inpatient Services, Artlink West Yorkshire, is a project reflecting the theme ‘We all make a difference.’
- The Red Kite Questionnaire Understanding Experiences of Services Together.
- Developing a Research Active Community, Leeds and York Partnership NHS Foundation Trust Research and Development.
- Gender Outreach Workers, supporting trans, non-binary and gender diverse people on the Leeds GIS waiting list, care pathway and people thinking about referral (18 plus).
- Leeds Perinatal Service, Peer Support Experience – Leeds Dads.
- Creative Writing at the Becklin Centre, Leeds Beckett University; Arts and Minds; and the Becklin Centre’s staff and service users.

Rounding up the day
Usmaan Khan, an expert with experience in services and Co-chair of the services network spoke about the day.
“I found it really nice, inspiring, and pleasant to see so many positive stories and developments going on in the Trust. I will continue to champion equity and equality, continue building the service user network, and hopefully try to bring more male and male-identifying people into co-production and involvement across the Trust.”
Les France, Lead Governor, talked about what he learned.
“What I’ve learned about our perinatal service and its amazing partner support, led by Errol Murray, has blown me away. What they do is amazing, and showcasing it is why we need days like this.” I’ve been inspired to “Ask many people we’ve heard from today to present to our governors. I’m sure they’d welcome the opportunity to hear about this inspirational work being done with our service users.”
Positive and Safe Working Group – Working together to reduce the use of restrictive practice
 The Positive and Safe Working Group (PaSWG) continues to lead our organisation’s commitment to reducing the use of restrictive practices. This includes minimising the use of blanket restrictions, physical restraint, seclusion, and emergency medication.
The Positive and Safe Working Group (PaSWG) continues to lead our organisation’s commitment to reducing the use of restrictive practices. This includes minimising the use of blanket restrictions, physical restraint, seclusion, and emergency medication.
Our Positive and Safe Care approach is a comprehensive framework designed to reduce reliance on restrictive interventions while ensuring the safety of both patients and staff. Central to this approach are proactive, preventative strategies such as Safewards and Positive Behavioural Support (PBS). These tools support the creation of positive and structured environments through clear expectations, consistent routines, and the development of trusting, collaborative relationships between staff and service users.
The Restrictive Interventions Annual Report shows encouraging progress across the Trust in 2024/2025, with a 14% reduction in physical restraints and a continued decline in the use of prone restraint across all inpatient services, despite ongoing challenges in certain areas. We remain especially focused on reducing high-level interventions such as prone restraint. For the second consecutive year, the use of prone restraint has continued to decline and now represents only 5% of all incidents involving physical restraint. Our goal is to continue reducing these figures even further in the year ahead.
Our Prevention and Management of Violence and Aggression (PMVA) training and education team plays a vital role in supporting this work. They have continued to review and develop staff training and are actively working to maintain our accreditation with the BILD Association of Certified Training. This accreditation reflects our strong commitment to delivering high-quality training that meets nationally recognised standards.
All staff working on our inpatient wards are required to complete annual PMVA training. This ensures they remain equipped with the most up-to-date skills and knowledge to manage challenging situations safely and effectively minimising the need for restrictive practices and prioritising the wellbeing of everyone involved.
Mental Health Legislation
The Mental Health Legislation Team is here to offer advice and support to staff, patients and carers in all matters relating to the Mental Health Act (MHA), Mental Capacity Act (MCA) and Deprivation of Liberty Safeguards (DoLS).
We ensure that staff receive the appropriate training and support and meet regularly with patients and carers to make sure they understand their rights under the Acts. We have completed audits in relation to consent to treatment certificates, use of holding powers and capacity assessments and best interest decision making. In response to the findings of these audits, the legislation team have put additional processes in place to support clinicians in making Second Opinion Appointed Doctor (SOAD) requests, developed an information leaflet for those considering an informal admission and have updated both the Mental Capacity Assessment and Best Interest Decision forms on Care Director.
Mental Health Act Managers (MHAMs)
Mental Health Act Managers (MHAMs) have a delegated responsibility to hear appeals and hold reviews of patients’ detentions. They are not employed by our organisation and are independent in their decision making. We are committed to ensuring that those carrying out this role reflect the diverse communities of our patient groups have complete significant recruitment to achieve this. We provide regular training for MHAMs to ensure that they are equipped for their role and hold a quarterly managers forum which is well attended.
Sexual Safety
![]() NHS England commissioned the National Collaborating Centre for Mental Health to develop standards and guidance on improving sexual safety in inpatient environments, following a report from the CQC in 2018 highlighting sexual safety incidents in inpatient areas. Here at our organisation, we are working hard to embed these standards. We have implemented the following to support sexual safety within our services, to keep staff, service users and visitors safe.
NHS England commissioned the National Collaborating Centre for Mental Health to develop standards and guidance on improving sexual safety in inpatient environments, following a report from the CQC in 2018 highlighting sexual safety incidents in inpatient areas. Here at our organisation, we are working hard to embed these standards. We have implemented the following to support sexual safety within our services, to keep staff, service users and visitors safe.
Sexual Safety Leads – each inpatient service across our organisation has a Sexual Safety Lead identified, to provide support and guidance in ensuring that the standards are met. We are working towards this within our Specialist and Community-based services.
The Sexual Safety Group – meets monthly, with membership including Sexual Safety Leads, Safeguarding professionals, Professional Lead Nurses, Quality & Patient Safety Leads, Heads of Clinical Governance, and any other clinicians or those in leadership roles who have a responsibility in maintaining sexual safety. The group also invite guest speakers to provide updates, information and support.
Sexual Safety Workshops – these have been provided to support the learning and development of Sexual Safety Leads and other clinicians within our services, for staff to develop confidence in preventing, responding to, and learning from sexual safety incidents.
PSIRF Local Priority – our organisation has identified Sexual Safety incidents affecting service users as a local priority in line with the new Patient Safety Incident Response Framework (PSIRF). This means that a learning response is required for all incidents related to sexual safety that have caused harm to a service user, with learning to be shared via the Sexual Safety Group, as well as service-level clinical governance arrangements.
Systems and Processes – work has also taken place to ensure that our systems and processes support accurate and timely reporting of any sexual safety incidents, with changes made to Datix (the incident reporting and risk management system used by our organisation) to reflect this so that incident categories are consistent, and data provided is accurate.
Training – training has been developed to ensure that staff across our organisation from all areas and disciplines understand the Sexual Safety Standards and are confident in reporting and responding to sexual safety incidents, as well as ensuring that service users are safe and protected from harm.
Information for service users – leaflets have been developed for service users, containing information on what sexual safety means, what they can expect from us to ensure that they are safe, and how to get help if they need it.
Oversight and Assurance – a quarterly report is produced, containing data relating to all sexual safety incidents reported across the organisation. The report identifies themes and trends, actions taken, and learning from incidents, and is shared and scrutinised at board level, as well as through the Sexual Safety group and clinical services.
The Sexual Safety Standards can be found on the Royal College of Psychiatrists website’s Sexual Safety Collaborative page.
Recognising Success
Positive Practice in Mental Health Awards
Our teams’ hard work and dedication to excellence were showcased at the Positive Practice in Mental Health Awards, highlighting the support we provide to our service users.
We were proud to have received eleven nominations across eight different categories, highlighting the breadth and depth of our commitment to delivering people-centred care. We are proud of the high-quality, specialist mental health, learning disability and neurodiversity services we provide.
We had 3 wins with our services and partner services, with many of our team’s work being highly commended.
Winners
- Children and young people’s mental health services – Red Kite View
- Mental health rehabilitation and/or recovery services – Joint winners Community Rehabilitation Enhanced Support Team (CREST)
- Specialist Services (including Veterans, Substance Misuse, Addictions, Housing, Education and Employment) – Op Courage
Highly commended
- Category Integrated Physical & Mental Health – Health facilitation team
- Category Learning Disabilities and/or Autism – Intensive support team
- Category Addressing Inequalities – Synergi Leeds and Gender Outreach Workers
- Category Acute inpatient care – Acute (Becklin) and Red Kite View
- Older adult functional mental health services and/or dementia care creative group projects – Older Peoples Service, the Mount
- Specialist Services (including Veterans, Substance Misuse, Addictions, Housing, Education and Employment) – North Assertive Outreach
Our Chief Exec makes the top 10 across the NHS
Dr Sara Munro, the Trust’s Chief Executive, was named as the 9th top Chief Executive in the NHS by the Health Service Journal.
The Health Service Journal (HSJ) released its ranking of 2024’s top Chief Executives, with Sara Munro being placed 9th out of 50. The HSJ recognises top leaders of NHS Trusts in England. Last year Sara made the top 50. The judges chose the top 50 based on three criteria: the performance of the organisation they lead, their contribution to the wider NHS, and the personal example they set. Although judges took individuals’ track records into account in the process, they also looked at CEOs’ focus for the next twelve months.
Sara has led the Leeds and York Partnership NHS Foundation Trust since 2016. She has worked extensively in mental health, with a background as a mental health nurse and clinical work in inpatient mental health settings. Sara is passionate about the needs of service users, carers, local communities, and staff and about ensuring their voices are heard in the decisions made about services.
In addition to her full-time role as Trust Chief Executive, Sara is also a senior leader within a wider group of Chief Executives and Chief Officers who come together to examine health and social care provision across Leeds and the whole of West Yorkshire. She acts as the Senior Responsible Officer for Mental Health, Learning Disabilities, and Autism within the West Yorkshire Integrated Care System.
In 2023 Sara was able to provide support and cover shifts during a period of extreme pressure and staff shortages within our community mental health service, as she’s still a registered mental health nurse.
Her experience has been a huge benefit for our services and her hands on approach to understanding the pressures they face.
On hearing the news, Sara said: “I feel very lucky to do a job I love and find rewarding and challenging. I work with the most amazing people every day in a sector that I have always felt deeply passionate about, and this inspires me to keep being who I am and focus on what matters to patients and staff.
She added: “It was a wonderful surprise to find out I have been named in the top 10 CEOs in the country. It reminds me to thank everyone who supports me and shares my passion every day.”
Ellen is recognised for her contribution to Leeds
 Ellen Scroop, Clinical Team Manager in Emerge Leeds Complex Emotional Needs Service had her name added to sculpture that celebrates women, both past and present, who have made a significant contribution to the city of Leeds.
Ellen Scroop, Clinical Team Manager in Emerge Leeds Complex Emotional Needs Service had her name added to sculpture that celebrates women, both past and present, who have made a significant contribution to the city of Leeds.
Created by artist, Pippa Hale, Ribbons is a sculpture that champions women’s achievements in Leeds. It was unveiled at its location at the top of the gardens between Leeds City College’s Quarry Hill campus and Leeds Playhouse at the gateway to the SOYO development at Quarry Hill.
Ribbons is comprised of five corten steel ribbons which carry the names of 383 nominated Leeds women. Ellen was nominated by six different people, a testimony to the esteem in which she is held.
Each woman recognised is listed on the sculpture’s website with background information on why she has been included, Ellen’s statement reads as follows:
Ellen Scroop has worked for over 20 years supporting community health in Leeds. She has made her mark on the city through pioneering work with the Probation Service and NHS, playing a key role in revitalising a struggling system of support for those with complex needs. Underpinning these successes is Ellen’s compassion, empathy and modesty, and a passion for achieving just and healthy communities. Ellen is an inspirational leader, advocate, friend and mother, a true unsung hero who is rarely in the spotlight despite her unwavering commitment to improving mental health across the city.
A celebration of Apprenticeship achievements at LYPFT
 Leeds and York Partnership NHS Foundation Trust (LYPFT) held the annual Apprenticeship Celebration Event on Friday 21 March 2025.
Leeds and York Partnership NHS Foundation Trust (LYPFT) held the annual Apprenticeship Celebration Event on Friday 21 March 2025.
We recognised the achievements of apprentices and those who supported them. We also celebrated those living the Trust’s values in our special Apprenticeship Awards. Colleagues were nominated for their ability to demonstrate Simplicity, Integrity, and Caring, with winners announced.
The Trust apprentices programme has grown, with 115 people currently enrolled and over 30 who have completed their programmes in the last 12 months. Opening the Apprenticeship celebration event, the Trust’s Chief Executive, Dr Sara Munro, remarked on the positive impact of the apprenticeship programme on both personal and professional development and its importance in improving service quality across the organisation. While acknowledging the support from line managers, mentors, and family members in their role in helping apprentices navigate their programmes alongside their day jobs.
Sara said: “Apprenticeships are a powerful tool for personal and professional growth. They not only enhance individual skills but also improve service quality across our organisation.”
Certificates were presented to the apprentices who had completed their programmes.
Improvement Made with Service User Involvement
Co-production in Community Mental Health Teams, Debbie Thrush, Clinical Lead
“Lived experience members of the Complex Trauma Involvement Group have been tasked with meaningful work – ‘distilling’ the often-complex message of trauma-informed care into something that will ‘resonate’ with; and hopefully motivate, the workforce. They additionally have a crucial role in overseeing implementation of a truly trauma-informed working culture. Several members of this group also co-presented at the three worker Introduction Days, as part of the Transformation launch.” Richard Barber, Trauma-Informed Lead for Transformation
“My involvement in ensuring that the Transforming Community Mental Health Services initiative is trauma-informed was deeply important to me because I know first-hand how crucial it is for services to truly understand and support those who have experienced trauma. Too often, mental health services can feel clinical or detached, failing to recognise the long-term impact of adverse childhood experiences and complex PTSD. By using my lived experience, I was able to advocate for a system that prioritises safety, empowerment, and genuine understanding—one that doesn’t retraumatise individuals, but instead helps them rebuild their lives with dignity and compassion. Being part of this work allowed me to channel my experiences into meaningful change, ensuring that others receive the kind of care and recognition that I once needed.
This involvement also gave me a sense of purpose and agency, transforming painful experiences into a driving force for improvement. It was empowering to know that my insights were valued and could influence real change in how mental health services are delivered. Trauma-informed care isn’t just about policies or training—it’s about shifting mindsets and creating environments where people feel truly heard and supported. Contributing to that shift meant that my voice, and the voices of many others with similar experiences, were no longer overlooked. It reaffirmed my belief that those who have lived through trauma are not just service users, but also experts in what truly works.” Ged Robinson, Lived Experience Member of the Complex Trauma Involvement Group.
“My desire to be involved in this project stems from a deep-rooted belief that true understanding, healing and transformation comes when we are supported to accept and acknowledge all parts of ourselves. Through this process I have been able to integrate my own experiences of trauma, service provisions and professional knowledge to advocate for a system of change. To be seen, heard and have my contributions towards this work valued and appreciated has been empowering. I have gained confidence showing up authentically and allowing my voice to be heard. To share spaces with others who have been impacted by trauma and to hear these expressed openly has been inspiring. There is power in vulnerability and together we have fostered deeper connection, empathy and understanding. There is hope that this translates into the wider working culture, supporting a trauma informed environment of safety, reflection and co-production.
We must acknowledge that we have all experienced ‘big T’ and ‘small T’ traumas which often have not been heard, expressed, or processed. To reframe our thoughts and experiences and heal we must first be supported to understand what has happened to us, complete the process, and release it. We must be seen and accepted in our entirety within a working culture that recognises the impact of trauma and strives to understand, support and empower us on our healing journeys. Placing the lived experience at the centre must be a priority. I hope that through hearing our voices it evokes reflection, learning and change. Together we can be the transformation we wish to see in the world.” Becca Gooding- Lived Experience Member of the Complex Trauma Involvement Group.
Guardian of Safe Working for Medical Staff
On the 1 February 2017 Leeds and York Partnership Foundation Trust transitioned all resident doctors onto the 2016 Resident Doctor Contract.
The Leeds and York Partnership NHS Foundation Trust Guardian of Safe Working (GoSW) was appointed in November 2016 and ensures that issues of compliance with safe working hours are addressed in line with the 2016 resident doctor contract. It provides assurance to the board that doctors’ working hours are safe. The GoSW has oversight of Exception Reports (ERs) and works closely with the Medical Education department (MEC). The GoSW also holds the position of Chair of the Resident Doctors Forum (RDF) which meets quarterly.
Doctors are encouraged to complete Exception Reports where there is variation from their work schedule or contracted working hours, to ensure appropriate review and action accordingly. No patient safety concerns have been raised from any Exception Reports, including those related to rota gaps within 2024/2025.
Patient Advice and Liaison (PALS), concerns, complaints and compliments
Our organisation’s Complaints and PALS Team provide a gateway to hear concerns and complaints about our organisation; and ensure they are managed in accordance with regulatory requirements.
We recognise that the formal complaints process is not always the best pathway for patients and families to receive a speedy resolution to a problem. We continue to promote a welcoming and positive culture for everyone contacting the PALS and Complaints Team.
During 2024/25, the Team dealt with 2719 PALS contacts, table 14 shows the number of complaints received compared with previous years.
Table 14.

Bar chart showing the number of PALS received each financial year from 2019/2020 to 2024/2025. The data indicates a general fluctuation over the years, with a notable increase in 2024/2025 reaching approximately 2600, the highest in the period shown.
Of the total PALS contacts received in 2024/25, 359 were concerns. The largest PALS type in 2024/25 was information request with 1139.
Themes of concerns tend to vary from formal complaints. Concerns are often problems that require immediate action such as meal options and environmental issues that the team are able to offer quick resolution.
The top three themes for all PALS contacts during 2024/25 were:
- Communication: 44%
- General Enquiry: 17%
- Clinical Treatment: 10%
85% of PALS contacts that were themed as communication were resolved within one day by providing advice/information or referring to a more appropriate department. It is important to note that PALS contacts are not always indicative of a concern. An example of a communication contact was an enquiry regarding apprenticeships. Although PALS is a patient focused service, it is responsive to any enquires, which are logged onto the Datix system.
In 2024/25, our organisation received 174 formal complaints. Table 15 below shows the comparison of complaints received over previous financial years.
Table 15.
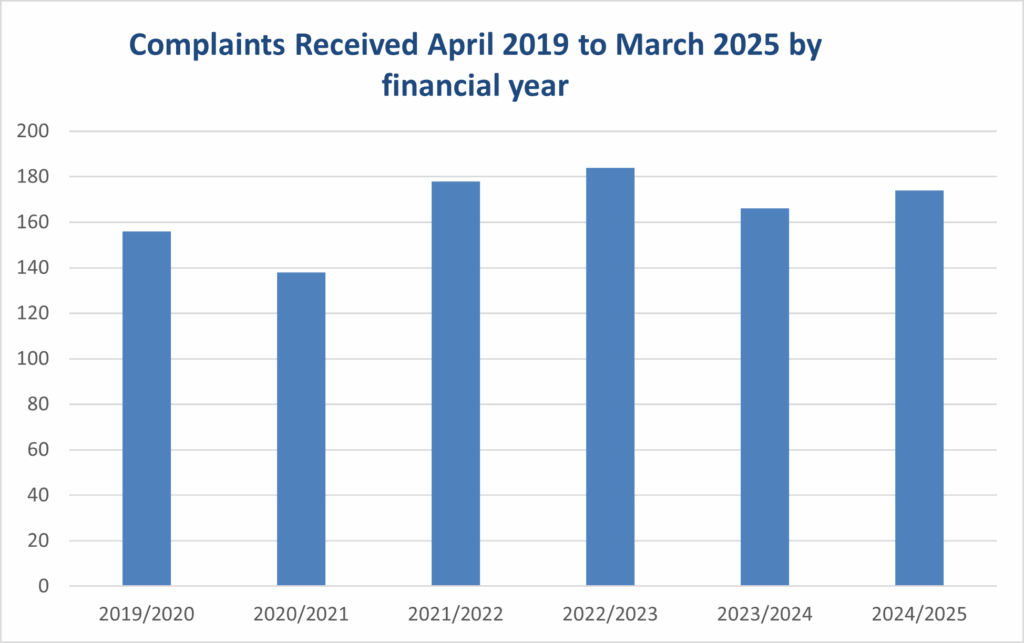
Bar chart illustrating the number of complaints received annually from 2019/2020 to 2024/2025. The data shows a peak in 2022/2023 with around 180 complaints, followed by a slight decline and then a modest rise again in 2024/2025.
Complaints present an opportunity for us to review care, our services; and the way in which we interact and provide information to our service users, from another perspective.
The top three themes for complaints during 2024/25 were:
- Clinical Care: 47%
- Admission, discharge and transfer: 22%
- Attitude of staff: 13%
Learning
As a Trust, we are committed to continuously improving and learning from complaints. The complaints team have made amendments to our reporting system and are now using it to manage actions from complaints. A complaint actions tracker is circulated to the clinical service lines on a quarterly basis. The complaints team continue to engage and support the Trust to use the learning from complaints effectively.
Learning examples of action implemented as an outcome of complaints received in 2024/2025:
- A complaint identified how communication styles and staff attitude impact on patients and their recovery. As a result, training sessions on Clinical Boundaries were held, led by the Professional Lead Nurse for the Trust.
- Knowledge and Understanding Framework Training was delivered to Ward staff to equip them with the confidence and skills to work effectively with service users who have a diagnosis of personality disorder or complex mental health needs.
- A complaint identified that the source of information contained within a discharge letter was not always clear i.e. information provided by the GP or family. This action was taken forward with the team reviewing the administrative process and amending the letter templates.
Key Achievements in 2024/25
- The PALS and Complaints Team have continued to work creatively to ensure that the team have been as accessible as possible to all service users and carers.
- The team have been working to streamline the complaints process ensuring that complaint reviewers are aware of the required tasks to take, ensuring good communication and updates are provided to our complainants.
- The development of a complaints tracker to ensure organisational oversight of open complaints has been further improved with the addition of the complaint action report. This report is circulated quarterly and enable oversight and assurance of actions.
Aims for 2025/2026
- Review and amend the complaint reviewer pack, to help support an improvement in the way complaints are handled.
- Further develop our training package offer, for those handling complaints.
- Further review and embed the process for complaint response actions and work with service lines to consider how learning and good practice from complaints is communicated trust wide.
- Align our data for PALS and complaints to the 3xCs themes (Communication, Coordination and Compassion) which is a recognised improvement programme across Leeds health and care organisations.
Compliments
Compliments are received for treatment, care, and support, in respect of our environment, atmosphere, and cleanliness. Staff can record all compliments received (either written or verbal) as well as being able to attach any cards/letters to our electronic DATIX reporting system.
During 2024/25, our organisation received 631 compliments. Compliments are a key measure of patient experience, and we are keen to develop recording of compliments alongside our other methods of feedback in order to create a fuller picture of where we are doing well and where we might be able to further improve.
These are some of the keywords of the compliments received in 2024/2025:
- Thank You
- Friendly
- Brilliant
- Felt Listened To
- Safe Space
- Positive
- Fantastic
- Informative
- Generous
- Valued
- Non Judgmental
- Impressive
- Reassuring
- Professional
- Attentive
- Consistent
- Understanding
- Respectful
- Genuine
- Patient
- Helpful
- Welcoming
- Grateful
- Supportive
- Caring
- Great
- Warmth
- Knowledge
Falls and Pressure Ulcer Management
Falls and pressure ulcers are reported by clinical staff on the Datix incident reporting system.
Falls resulting in moderate or high harm and all pressure ulcers are discussed at the Trust Falls and Pressure Ulcer Improvement Forum (FAPU). The aim of discussions at FAPU is to identify learning and support improvement work.
Reported Falls
In 2024/25 the Trust reported 491 falls incidents across the inpatient, specialist supported living settings and community services.
Table 16 – Number of reported falls by Quarter and level of harm.
| Reported Falls | No harm | Low harm (Minimal harm required extra observation or minor treatment) | Moderate harm (Short term harm required further treatment or procedure) | Severe harm (Permanent or long-term harm) |
| Quarter one | 96 | 28 | 2 | 0 |
| Quarter two | 87 | 35 | 6 | 0 |
| Quarter three | 85 | 33 | 4 | 0 |
| Quarter four | 83 | 31 | 0 | 1 |
| Totals | 351 | 127 | 12 | 1 |
Overall total of reported falls: 491.
Pressure Ulcers
All pressure ulcers and moisture associated skin damage identified by Trust staff are reported as incidents. Whilst the Trust sees relatively few pressure ulcer incidents, their cause and management can be complex and closely linked with a person’s mental health or learning disability presentation. Table 17 below shows the distribution of reported pressure ulcers which developed or deteriorated under the care of the Trust (as a primary provider of care) by level of harm over each quarter.
Table 17 – Number of reported pressure ulcers by Quarter and level of harm.
| Reported pressure ulcers | No harm | Low harm (Minimal harm required extra observation or minor treatment) | Moderate harm (Short term harm required further treatment or procedure) | Severe harm (Permanent or long-term harm) |
| Quarter one | 0 | 0 | 2 | 0 |
| Quarter two | 0 | 0 | 4 | 0 |
| Quarter three | 0 | 0 | 5 | 0 |
| Quarter four | 0 | 0 | 1 | 0 |
| Totals | 0 | 1 | 12 | 0 |
Overall total of reported pressure ulcers: 13.
Examples of improvement work
- Lying and Standing Blood pressure assessment is now part of the admission procedure on all the older peoples’ wards. This is in line with best practice as an evidence-based falls prevention measure.
- Development of a specialist falls fact find, as part of the implementation of PSIRF in the Trust. A trial of this fact find is currently underway and will be evaluated before implementation.
- A multi-disciplinary sub-group of FAPU is developing a multi-factorial falls assessment to be used with all service users who are at high risk of falls. This will be in line with NICE guidance on falls prevention (guidance to be published March 25).
- Proposed increase in physiotherapy provision at the Mount to improve falls prevention assessment and interventions.
- Physical Health Inreach Team (PHIT) with Care Director team to develop guide on completion of the PURPOSE-T PU risk assessment tool to support improvement of the use of this across trust based on feedback from clinical staff and the FAPU.
- Bite sized PU training has been delivered by the PHIT including acute service and OPS preceptees and support staff around PU prevention, recognition treatment and pathways.
- In July, a review of the PU prevention procedure instigated by new national safeguarding guidance. Following this the PU prevention policy was approved at the Policy and Procedure meeting.
Section Four
Statements from Others on the Quality Account
Leeds and York Partnership NHS Foundation Trust Quality Account 2024-25 from Healthwatch Leeds
Thank you for this opportunity to comment on your Quality Account. We are happy to see that it shows a lot of focus on how people’s experiences have been taken into consideration in improving the services that the Trust provides.
We work closely with the LYPFT Patient and Carer Experience Team who are key members of the People’s Voices Partnership (PVP) as well as the How Does It Feel For Me working group. They are joined with us in the aim of putting people’s experiences at the centre of health and care decision making. It is great to see that the Trust’s aims for 2025/26 is to align their data with the 3Cs (Communication, Coordination and Compassion). We are happy to work with the Trust and the wider partnership on this and look forward to hearing more about the implementation of this.
Mental health support is one of the main issues that we hear from people and communities about at Healthwatch Leeds. Therefore, LYPFT have an important role as one of the main providers of secondary mental health care in Leeds. This Quality Account has good intentions but has limited evidence in people’s experiences. There are positive examples used such as co-producing care plans, gathering feedback through ‘Have Your Say’ and involving 82 service users in 66 projects. There are gaps however such as limited detail on impact, delays in patient safety partner schemes, and missed opportunities to showcase learning from complaints and service user suggestions.
The past year has seen a big shift in service change with the closure of the Single Point of Access (SPA) for people in crisis which has moved to an option on NHS 111. It is disappointing to see that this has only been referenced lightly and in the Quality Account there is no reference to the impact of this change on people. We have recently done a piece of work to understand what people’s experiences of this change have been. We hope to work with the Trust to improve people’s experiences.
It is good to see a section on inequality/equity and that equity is clearly a priority which has been highlighted in the CEO’s message, strategic goals and in specific projects. Efforts include plans to reduce health inequalities, new Health Equity Fellows, inclusive chaplaincy work, and a race equality framework focused on co-production. However, not too much has been done yet to implement the plan nor the outcomes of projects such as Synergi and anti-racism measures. It would also be great to see the Trust move into the co-design space. We look forward to seeing what happens over the next year.
The Quality Account has some use of clear language, but the style feels inconsistent, and acronyms are not always explained fully. The Quality Account mentions that it has been seen by service users and concerns have been listed. There is no direct mention of actions taken to address these concerns. It is also notable that that people’s experience is mentioned, but not well integrated into the quality reporting. It would be incredible to see the adoption of the 3Cs (Communication, Coordination and Compassion) within this.
Overall, the Quality Account demonstrates a commitment to involving people with experience and addressing health inequalities. There are encouraging examples of co-production, engagement with people and a strategic focus on equity. However, the Account often falls short of clearly showing how people’s feedback has led to tangible improvements in services. While key values and priorities are stated, the impact of service user involvement is not always well-evidenced. Several initiatives lack detail or follow-up, and suggestions from previous feedback appear to have been overlooked. To strengthen future reports, clearer evidence of outcomes, improved consistency in style, and better integration of people’s input would be beneficial. At Healthwatch Leeds, we look forward to the opportunity of working with Leeds and York Partnership NHS Foundation Trust and partners across the city more closely to ensure that people are at the centre of health and care decision making and delivery.
The Integrated Care Board in Leeds Review of Leeds and York Partnership Foundation Trust Quality Account 2024/2025
Abby Boden
Head of Clinical Governance
Leeds and York Partnership NHS Foundation Trust Trust Headquarters
Main House
St Mary’s House Leeds
LS7 3JX
19 May 2025
RE: The Integrated Care Board in Leeds Review of Leeds and York Partnership Foundation Trust Quality Account 2024/2025.
Dear Abby,
The Integrated Care Board (ICB) in Leeds is pleased to review the Leeds and York Partnership Foundation Trust (LYPFT) Quality Account 2024/2025. The ICB in Leeds acknowledge that the report is still in draft form and some additional information may still need to be added prior to final publication, so please accept our observations on that basis.
The Quality Account is comprehensive and accessible, with clear language and well- chosen images and illustrations that enhance the text and support reader engagement. It demonstrates a strong emphasis on capturing the voices of patients and carers, showing how their feedback informs service development and drives improvement. The report also highlights the excellent partnership working between the Trust and the local community, showcasing the wide range of specialist and complex services delivered daily to the people of Leeds.
The detail provided around the Trust’s 2024/25 Quality Improvement Priorities (QIPs) is both informative and engaging. The three strategic priority areas demonstrate a strong focus on patient safety and align closely with national objectives, particularly in reducing health inequalities and enhancing the quality of care. The Quality Account clearly articulates each priority, offering a well-structured overview of the Trust’s progress against each of their priorities, while effectively conveying the vision and aims behind each initiative.
The inclusion of the Patient and Carer Race Equality Framework (PCREF) is highly commendable. The Trust’s progress as an early adopter of this framework is both encouraging and reflective of its strong commitment to becoming a fully inclusive provider. It is clear that co-production is central to the Trust’s approach, alongside a clear and meaningful ambition to become an actively anti-racist organisation.
It is reassuring to see that the Trust will continue to prioritise these Quality Improvement Priorities (QIPs) in the coming year, ensuring they are fully embedded across the organisation and that momentum in these key areas is sustained.
It’s clear that the Trusts Quality Strategic Plan 2025 & Beyond will continue to underpin the Trust’s strategic plans and commitment to improving quality of care. LYPFT is actively embedding the STEEEP principles of Safe, Timely, Effective, Efficient, Equitable, and Patient-centred care into its approach to quality improvement. These principles will guide service development, support continuous improvement, and ensure that patient care is consistently aligned with best practice standards. By applying STEEEP, LYPFT is fostering a culture that prioritises safety and clinical effectiveness while also recognising the importance of personalisation, accessibility, and reducing variation in outcomes. This structured approach reflects the Trust’s commitment to delivering high-quality care that meets the diverse needs of the communities it serves.
The focus on enhancing people’s experiences, as evidenced by involving people with lived experience in the development of this quality account, is exemplary and aligns closely with our values. This is a strong example of how people who use services can become closely involved and be part of shaping their own services. The addition of the information about the work of the Patient and Carer Experience Team and the Service User Network further demonstrates that the organisation cares strongly about being inclusive and fully understanding the views and experiences of patients. It’s encouraging to hear about this work and specifically how the topics discussed within these groups and networks are directly influencing quality and improvement of services.
The ICB in Leeds would like to thank LYPFT for sharing their Quality Account 2024/25 with the ICB in Leeds. We appreciate the time and effort taken to produce such a comprehensive and engaging report. It clearly reflects your ongoing commitment to quality, patient involvement, and continuous improvement. We would also like to take this opportunity to thank you for your hard work and achievements throughout 2024/25, and we look forward to continuing our collaborative work to support the people of Leeds and strengthening our partnership going forward.
Yours sincerely,
Rebecca Walker Quality Manager
West Yorkshire Integrated Care Board in Leeds
Acknowledgements
We would like to sincerely thank everyone who contributed to the content and publication of our 2024/2025 Quality Account. This includes, but is not limited to, service users, carers, and representative groups, many of our staff, service and Professional Leads, the Senior Management Team and the Board of Directors.
This document provides an insight into how we are working to realise our values, our strategies, and plans for these; and our aim to continually improve, which is at the heart of everything we do. We hope you find the document to demonstrate this and have enjoyed reading about the quality of our services.
Glossary
Allied Health Professional (AHP)
Comprises of distinct occupations including art therapists, dietitians, music therapists, occupational therapists, physiotherapists, and speech and language therapists.
Appraisal
A method of reviewing the performance of an employee against nationally agreed standards within the NHS.
Audit
A review or examination and verification of accounts and records (including clinical records).
Board of Directors
The team of executives and non-executives who are responsible for the day to day running of an organisation.
Care Quality Commission (CQC)
The independent Health and Social Care regulator for England.
Clinical Coding
An electronic coded format that describes the condition and treatment given to a patient.
Clinical Governance
The framework through which healthcare organisations are accountable for continuously improving the quality of their services and safeguarding high quality of care.
Clinical Supervision
A reflection process that allows clinical staff to develop their skills and solve problems or professional issues. This can take place on an individual basis or in a group.
Community Mental Health Team (CMHT)
Support people living in the community who have complex or serious mental health problems.
Continuous Improvement (CI)
A management approach that organisations use to reduce waste, increase efficiency, and increase internal (employee) and external (customer/patient) satisfaction. It is an ongoing process that evaluates how an organisation works and ways to improve its processes.
CQUIN (Commissioning for Quality and Innovation)
A financial incentive encouraging Organisations to improve the quality of care provided.
Datix
An electronic risk management system (database) used to record incidents, complaints, and risks for example.
DOLS (Deprivation of Liberty)
DoLS protect people who lack capacity to consent to being deprived of their liberty. This means that because an illness, an injury or a disability has affected the way their mind works they are not able to agree that they will not be allowed to do certain things.
Duty of Candour (DoC)
A legal duty on hospital, community, and mental health organisations to inform and apologise to patients if there have been mistakes in their care that have led to harm.
E-Rostering
An electronic staff management tool used to plan staff requirements and reported on staff hours worked, annual leave, sickness etc.
IHI
The Institute for Healthcare Improvement takes a unique approach to working with health systems, countries, and other organizations on improving quality, safety, and value in health care.
Information Governance
The rules and guidance that organisations follow to ensure accurate record keeping and secure information storage.
Inquest
A judicial inquiry to ascertain the facts relating to an incident.
LD
Learning Disability: a reduced intellectual ability and difficulty with everyday activities – for example household tasks, socialising or managing money – which affects someone for their whole life.
LIMM
Learning from Incidents and Mortality Meeting
Legislation
A law or set of laws suggested by a government and made official by a parliament.
Learn from Patient Safety Events (LFPSE)
LFPSE is a national NHS service for the recording and analysis of patient safety events that occur in healthcare.
MAPPA
Multi Agency Public Protection arrangements
Medicines management
Processes and guidelines which ensure that medicines are managed and used appropriately and safely.
Mental Health Act (1983)
The main piece of legislation that covers the assessment, treatment, and rights of people with a mental health disorder. People detained under the Mental Health Act need urgent treatment for a mental health disorder and are at risk of harm to themselves or others.
Methodology
A system of methods used in a particular area of study or activity.
NHS England (NHSE)
The central organisation that leads the NHS in England and sets the priorities and direction of the NHS.
National Institute for Health and Care Excellence (NICE)
An organisation that provides national guidance and advice to improve health and social care with the aim of improving outcomes for people using the NHS and other public health and social care services.
National NHS staff survey
A survey that gathers the views of staff working in the NHS to give an overall indication of their experience of working for the NHS.
Non-medical Responsible Clinician
Traditionally, only psychiatrists could be an Approved Clinician, (sole responsibility for the overall care and treatment of someone detained under the Mental Health Act). In 2007 amendments were made enabling non-medics, such as nurses, social workers, psychologists and occupational therapists, to become Approved Clinicians.
Outcome Measures
A measure (using various tools) of the impact of the intervention from a clinician’s perspective or a measure of progress related to a specific condition or issue.
Patient acuity
A measure of the severity of illness of the patient and the intensity of nursing care that patient requires.
Patient Advice and Liaison Service (PALS)
A service that provides a listening, enquiry and signposting service to ensure that patients, carers and public have their questions and concerns resolved as quickly as possible.
Patient experience
Feedback from patients on ‘what happened and how they felt’ in the course of receiving their care or treatment.
Patient satisfaction
A measurement of how satisfied a person felt about their care or treatment.
Payment by results
The system applied to some services whereby NHS providers are paid in accordance with the work they complete.
Preceptee
A person undergoing preceptorship (see below).
Preceptor
An experienced member of staff who provides role support and learning experiences to the preceptee to assist them acquire new competencies.
Preceptorship
A structured period of transition for a newly qualified member of clinical or therapy staff when then begin their employment in the NHS.
Pressure ulcer
Damage caused to the skin and the tissue below when it is placed under enough pressure to stop the blood flowing.
Psychological
A mental or emotional rather than a physical cause.
Public Health England
An organisation that works to protect and improve national health and wellbeing and reduce health inequalities.
Quality improvement methodology
A systematic approach using specific methods to improve quality, achieving successful and sustained improvement. Through changing provider behaviour and organisation through using a systematic change method and strategies.
Risk Assessment
A process to identify risks and analyse what could happen as a result of them.
Serious Incident (SI)
When a patient, member of staff (including those working in the community), or a member of public suffers injury or unexpected death, or the risk of death or injury in hospital, or health service premises or other premises where healthcare is provided or where actions of health service staff are likely to cause significant public concern.
Strategy
The overall plan an organisation has to achieve its goals over a period of time.
Structured Judgement Review (SJR)
Used to effectively review the care received by patients who have died. This will in turn allow learning and support the development of quality improvement initiatives when problems in care are identified.
Specialist Thematic Review (STR)
A Specialist Thematic Review involves a comprehensive analysis of a specific topic or theme across different healthcare settings to identify patterns, understand the root causes of issues, and develop solutions for improvement. These reviews often use qualitative data like incident reports and feedback to uncover safety issues and guide future safety improvements.
Subject Access Requests (SAR)
Requests made for personal information under the Data Protection Act 1998.
Standard Operating Procedure (SOP)
A set of step-by-step instructions compiled by an organisation to help workers carry out routine task.
Contact us
Leeds and York Partnership NHS Foundation Organisation
Telephone: 0113 85 55000
Organisation Headquarters
Main House St Mary’s House
St Mary’s Road,
Leeds
LS7 3JX
Chief Executive
If you’d like to get in touch with Dr Sara Munro, our Chief Executive, please call
Telephone: 0113 85 55913
You can follow Sara on X (Twitter): @munro_sara
Communications
For all media enquiries or if you would like copies of the Quality Account or more information about the Organisation you can contact us on:
Tel: 0113 85 55989
Patient Advice and Liaison Service (PALS)
Tel: 0800 052 5790
Email PALS
Let’s get social!
Follow the Trust on:
Page last updated: 11th Jul 2025 10:32am